
 ">
">
The Research Council of Norway, a funding partner in the Population and Poverty Research Network (PopPov) for which PRB is the Secretariat, recently hosted a knowledge-sharing event at the Norwegian Agency for Development Cooperation (Norad) in Oslo, Norway. To accommodate policymakers’ busy schedules, the Research Council challenged each presenter to discuss their research results, policy implications, and recommendations in six minutes or less.
The Research Council staff knew that researchers pay great attention to detail and to research nuances that could not be included in the short presentations, but they wanted to encourage policymakers to attend the presentations and to ask questions. At the conference, “A Gender Perspective on Demography and Conflict,” researchers explained the complexity of local circumstances in which women act strategically to access reproductive health care, to generate income, to care for their children, and to access legal rights. There was also a session on women and gender equality focusing on woman and conflict.
The researchers accepted the “speed presentation” challenge with varying degrees of enthusiasm. In the end, their commitment was clear: They all presented complex research studies and implications in less than seven minutes. PRB coordinated coaching and a rehearsal in the days leading up to the conference, helping research teams focus their messages and streamline their PowerPoint slides. PRB staff also wrote a brief summarizing results from ECONPOP (Economic Growth, Poverty Reduction, Reproductive Health, and Population Dynamics), a research program that has contributed to understanding interactions among poverty, cultural conditions, and reproductive health in sub-Saharan regions of Africa and in Nepal.
Communication with stakeholders is a common mandate of the Research Council of Norway and PRB. The two organizations also have a mutual interest in results presented by researchers from ECONPOP.
The ECONPOP projects contributed new knowledge relevant to achieving universal primary education (MDG 2); promoting gender equality and women’s economic empowerment (MDG 3); reducing child mortality (MDG 4); and improving reproductive and maternal health (MDG 5). The program targets all these goals in order to address the multiple dimensions of income and poverty in low-income countries. Laila Bokhari, Norway’s State Secretary at the Ministry of Foreign Affairs, who opened the conference, emphasized her country’s role as a leader in women’s reproductive rights and empowerment and their continued commitment to research.
ECONPOP is the result of a collaboration between the Research Council of Norway, Norad, and The William and Flora Hewlett Foundation. ECONPOP is also part of a larger initiative that has been supported by the Hewlett Foundation from 2005 to 2015: The Population and Poverty (PopPov) Research Initiative.
Kathy Bonk of Communications Consortium Media Center and Marlene Lee and Meredith Pierce of PRB reviewed research slides and conducted coaching sessions for presenters.
(April 2001) Europe has the lowest fertility rates in the world. In 2000, the average for the region was 1.4 children per couple, and it ranged from 1.1 children in Bulgaria and the Czech Republic to 2.2 children in Albania.
Social scientists posit a number of explanations for Europeans’ apparent reluctance to have children. Many point to the rising costs of raising children — not just higher costs of living, but also the personal costs to parents of deferred professional advancement and individual fulfillment. Another explanation focuses on related changes in social expectations about marriage and family formation: Young Europeans may not feel the same social pressure to get married and have children as did their parents and grandparents.
Europe’s low fertility has also been linked to the so-called “contraceptive revolution.” There is a common assumption that access to effective contraception is universal in Europe and that European women can successfully control if and when they get pregnant. Until recently, however, there was little empirical evidence about contraceptive use among European women. In the 1990s, a series of national surveys revealed new information about the level of contraceptive use and the most popular methods in various countries. The surveys also show that European women still have surprise pregnancies, despite the easy availability and high contraceptive use rate. (See Box below.)
The vast majority of European women of childbearing age use contraception — and Europeans are more likely than Americans to be practicing birth control. In most European countries, more than four out of five women of childbearing age who were married or in a marriage-like relationship were using a contraceptive method at the time of the survey. The use rates ranged from 92 percent in Hungary in 1993, to 66 percent in Lithuania in 1995 (see Table 1). A 1995 survey in the United States showed that three-quarters (75 percent) of currently married American women ages 15 to 44 were using a contraceptive method; 69 percent of formerly married American women were using a method.
Table 1
Contraceptive Use in Selected European Countries, 1990
| Country/ Year of survey | Percent of women in union using contraception |
|---|---|
| Austria, 1996 | 67.9 |
| Belgium, 1992 | 84.2 |
| Finland, 1990 | 84.0 |
| France, 1994 | 89.9 |
| Germany, 1992 | 84.8 |
| Hungary, 1993 | 91.8 |
| Latvia, 1995 | 84.9 |
| Lithuania, 1995 | 65.9 |
| Norway, 1989 | 80.3 |
| Poland, 1991 | 75.7 |
| Slovenia, 1995 | 84.4 |
| Spain, 1995 | 87.2 |
| Canada, 1995 | 80.2 |
| United States*, 1995 | 76.4 |
* Currently married women ages 15 to 44. Note: The percentage is based on a sample of women of reproductive age who were in union and therefore exposed to the risk of pregnancy. The ages of respondents varied by country. Most surveys included women 20 to 45; some surveys also included slightly younger and older women.
Sources: Author’s calculations of data from the Fertility and Family Surveys; and J. Abma, A. Chandra, W. Mosher, L. Peterson, and L. Piccinino, “Fertility, Family Planning, and Women’s Health: New Data from the 1995 National Survey of Family Growth,” Vital and Health Statistics Series 23, no. 19 (Hyattsville, MD: National Center for Health Statistics, 1997): Table 42.
The nearly universal use of contraception in Europe today is a phenomenon that appeared in the past three decades. Only one-third of European women born in the 1940s and 1950s used contraception the first time they had sex, for example, while more than two-thirds of women born in the 1970s used contraception the “first time.”
Most European women rely on highly effective contraceptive methods. Oral contraceptives are the most popular form of birth control; the pill is particularly dominant in Germany where it accounts for 84 percent of contraceptive use (see Table 2). Female sterilization, which rivals the pill as the top method in the United States, is not as popular in Europe. Sterilization was important only in Belgium, Spain, and Finland, where it accounted for 10 percent to 18 percent of use.
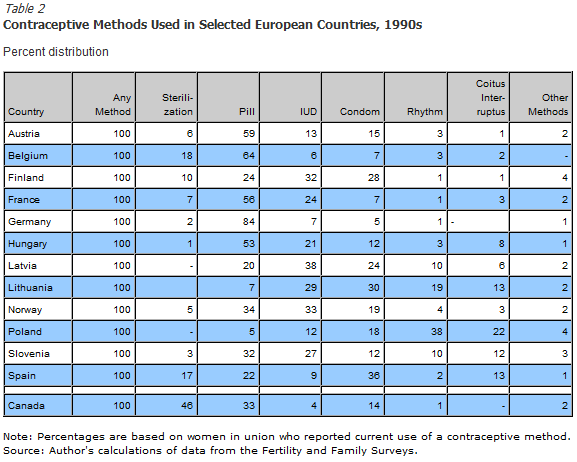
Surprisingly, traditional methods that have a relatively high failure rate are still widely used, especially in Spain and Eastern Europe. In Poland, more than one-third of women in a marital union reported using the rhythm method, while more than one-fifth said they used withdrawal. Rhythm (or periodic abstinence) and withdrawal (“coitus interruptus”) are the only forms of birth control condoned for married couples by the Catholic Church. This religious sanction might explain the higher use rates for these methods in countries like Poland and Lithuania that have large Catholic populations. Another barrier to the use of the pill or other “supply” methods in former Soviet countries, including Latvia, Lithuania, and Poland, was that the importation of contraceptives was often limited and many women did not have a reliable source of supply.
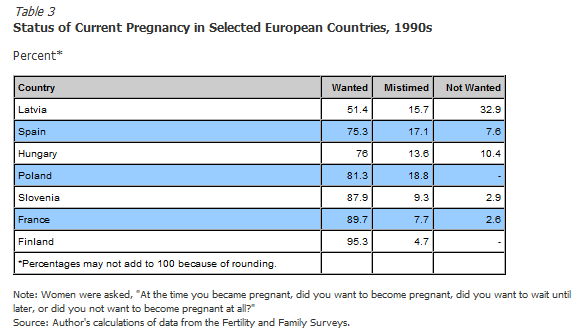
The efficiency of contraceptive methods used vary from country to country, in part reflecting the reliability of supply and consistency of use. Contraceptive failure is starkly reflected in measures of unwanted pregnancy. Nearly one-half of Latvian women and more than one-fifth of Hungarian and Spanish women pregnant at the time of the survey said they had not wanted their current pregnancy, or had wanted it at a later time (see Table 3). In France this share was 10 percent; in Finland, it was only 5 percent. In a 1995 survey in the United States, by comparison, about 9 percent of pregnancies were unwanted at the time of conception. A much larger share of pregnancies (21 percent) were “mistimed,” according to U.S. women interviewed.
How can European women avoid unwanted pregnancies? Better information and education on reproductive health could help. Despite high levels of formal education, some women still have gaps in their knowledge about when they are fertile or how to use contraceptives effectively.
Reducing unwanted pregnancies would prevent many abortions, which many people consider a laudable goal — abortion is quite prevalent in some Eastern European countries. Eliminating unwanted pregnancies would also reduce fertility, however, which is not a popular outcome. Most Europeans would not welcome lower fertility rates.
Ralf Ulrich is president of Eridion, GmbH, based in Germany.
Box
Collecting Information on Contraceptive Use in Europe
Until recently, there has been more information on contraceptive use and family planning in less developed countries in Asia, Latin America, and Africa than there has been in Europe. There have been several series of national surveys administered in less developed countries since the 1970s, fueled by the apparently urgent need for information about childbearing and family planning in countries where women had five to six children, on average, and where population growth was outstripping economic growth. The most recent and extensive effort is the Demographic and Health Survey (DHS) project, which involves more than 140 surveys in nearly 70 countries. But there has been less urgency about family planning behavior in Europe, where women appeared to have control over their reproductive lives and fertility was low. Only a few countries in the region conducted national surveys before the 1990s.
In the 1990s, a series of fertility surveys known as the Fertility and Family Surveys (FFS) were conducted in 24 more developed countries, primarily in Europe. The national surveys of 1,700 to 6,000 women (depending on the country) are an important source of information about contemporary patterns in the use of contraception in Europe. The questionnaires covered a broad range of problems related to fertility and family formation; many of the surveys also included a questionnaire for men. The minimum ages of respondents were not uniform, however. In most surveys, the ages of respondents ranged from 15 to 24 at the lower end, and from 40 to 49 at the upper end.
The design of the FFS benefited from the experiences with the DHS in less developed countries. Implementing the FFS questionnaires showed, however, that it was much more difficult to use standardized questionnaire modules in Europe than in the DHS countries. Consequently, FFS survey data on contraceptive use and other variables are less comparable than DHS data sets. Published individual country reports differ substantially in the way contraceptive prevalence is computed, but they provide a benchmark for further research into childbearing and family planning in Europe.