Farzaneh Roudi-Fahimi
Former Director, Middle East and North Africa

The people of the Middle East and North Africa (MENA) have long played an integral, if sometimes volatile, role in the history of human civilization. MENA is one of the cradles of civilization and of urban culture. Three of the world’s major religions originated in the region — Judaism, Christianity, and Islam. Universities existed in MENA long before they did in Europe. In modern times, MENA’s politics, religion, and economics have been inextricably tied in ways that affect the globe. The region’s vast petroleum supply — two-thirds of the world’s known oil reserves — is a major reason for the world’s interest. But the influence of MENA extends beyond its rich oil fields. It occupies a strategically important geographic position between Asia, Africa, and Europe. It has often been caught in a tug-of-war of land and influence that affects the entire world.
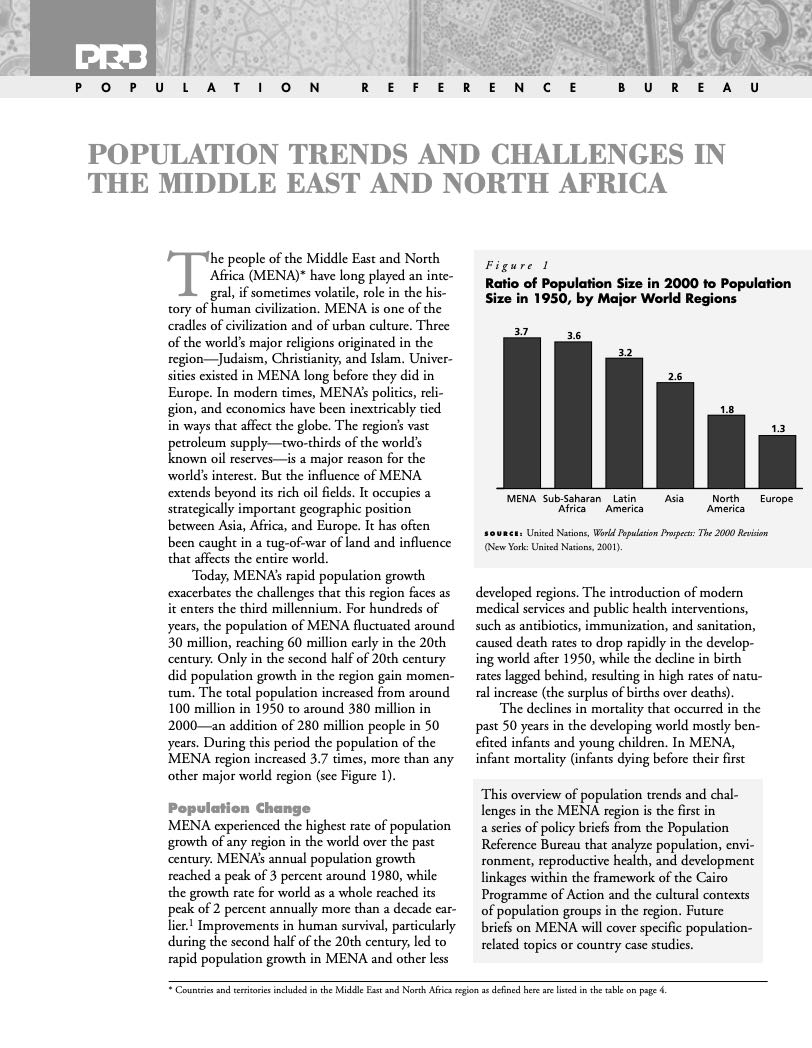
Today, MENA’s rapid population growth exacerbates the challenges that this region faces as it enters the third millennium. For hundreds of years, the population of MENA fluctuated around 30 million, reaching 60 million early in the 20th century. Only in the second half of 20th century did population growth in the region gain momentum. The total population increased from around 100 million in 1950 to around 380 million in 2000 — an addition of 280 million people in 50 years. During this period the population of the MENA region increased 3.7 times, more than any other major world region (see Figure 1).
Figure 1
Ratio of Population Size in 2000 to Population Size in 1950, by Major World Regions
Source: United Nations, World Population Prospects: The 2000 Revision (New York: United Nations, 2001).
MENA experienced the highest rate of population growth of any region in the world over the past century. MENA’s annual population growth reached a peak of 3 percent around 1980, while the growth rate for world as a whole reached its peak of 2 percent annually more than a decade earlier.1 Improvements in human survival, particularly during the second half of the 20th century, led to rapid population growth in MENA and other less developed regions. The introduction of modern medical services and public health interventions, such as antibiotics, immunization, and sanitation, caused death rates to drop rapidly in the developing world after 1950, while the decline in birth rates lagged behind, resulting in high rates of natural increase (the surplus of births over deaths).
The declines in mortality that occurred in the past 50 years in the developing world mostly benefited infants and young children. In MENA, infant mortality (infants dying before their first birthdays) dropped from close to 200 deaths per 1,000 live births in the early 1950s to fewer than 50 deaths per 1,000 live births at the turn of the 21st century. Despite this sharp decline and the fact that infant mortality rates in some oil-rich Persian Gulf states are quite low (Kuwait’s infant mortality is as low as the average for Europe), the regional infant mortality rate in MENA remains higher than that of Latin America and East Asia (see Figure 2).
Figure 2
Decline in Infant Mortality
Source: United Nations, World Population Prospects: The 2000 Revision (New York: United Nations, 2001).
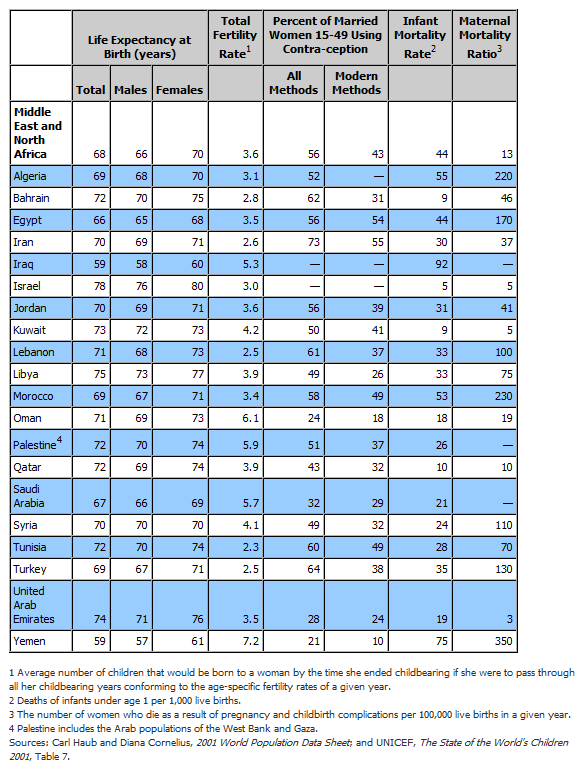
While the “demographic transition,” the shift from high to low mortality and from high to low fertility, is well under way throughout the region, individual countries are at different stages (see Figure 3). On average, fertility in MENA declined from 7 children per woman around 1960 to 3.6 children in 2001. The total fertility rate (average number of births per woman) is less than 3 in Bahrain, Iran, Lebanon, Tunisia, and Turkey, and is more than 5 in Iraq, Oman, Palestinian Territory, Saudi Arabia, and Yemen (see Table 1).
Figure 3
Total Fertility Rates
Countries and territories included in the Middle East and North Africa region as defined here are listed in Table 1.
Source: United Nations, World Population Prospects: The 2000 Revision (New York: United Nations, 2001).
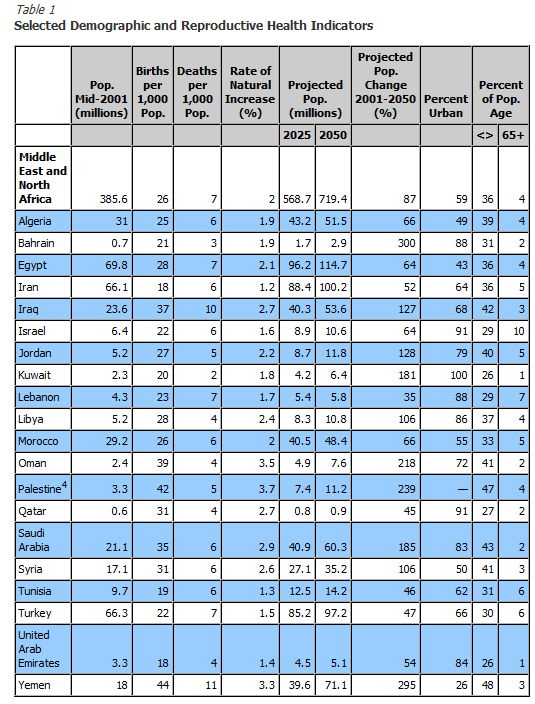
Even though the decline in fertility rates is expected to continue in the MENA region, the population will continue to grow rapidly for several decades. In a number of countries, each generation of young people enters childbearing years in greater numbers than the previous generation, so as a whole they will produce a larger number of births. This phenomenon is referred to as “population momentum.” The population of the region is increasing at 2 percent per year, the second highest rate in the world after sub-Saharan Africa. Nearly 7 million people are added each year, and MENA’s population is expected to nearly double in the next 50 years (see Figure 4).
Figure 4
Ratio of Projected Population Size in 2050 to Population Size in 2001
* Palestine includes the Arab populations of the West Bank and Gaza.
Source: Carl Haub and Diana Cornelius, 2001 World Population Data Sheet (Washington, DC: Population Reference Bureau, May 2001).
Regardless of the level of economic development or national income, MENA governments are increasingly challenged to provide the basic needs for a growing numbers of citizens — adequate housing, sanitation, health care, education, and jobs — and to combat poverty, narrow the gap between rich and poor, and generally improve the standard of living. In addition, the region’s scarce water resources need to be managed in the face of growing demand.
Its young population gives unprecedented momentum to MENA’s population growth. One-third of MENA’s population is under age 15. Over the next 15 years these children and adolescents will reach their childbearing years and enter the job market. In most MENA countries, the number of women of childbearing age (15 to 49 years) will at least double in the next 30 years. Providing quality reproductive health services to a growing number of women is a challenge and is key to slowing population growth.
As MENA’s total population increases, so does its elderly population and with it a health burden that has important implications for the cost and configuration of health systems. For example, the elderly population of Egypt (60 years and older) is expected to grow from 4.3 million in 2000 to 23.7 million in 2050. Saudi Arabia’s elderly population is expected to grow from 1 million in 2000 to 7.7 million in 2050.
MENA’s working-age population is growing very rapidly as huge cohorts of children reach adulthood. In 1996, for example, there were five Jordanians under 15 years of age poised to enter the labor market for every Jordanian age 45 to 60 nearing retirement age. For Saudi nationals, this ratio was 8-to-1 in 1996 (see Figure 5).
Figure 5
Age and Sex Profiles of Jordan and Saudi Arabia in Mid-1990s
Source: United Nations Economic & Social Commission for Western Asia (ESCWA), Demographic and Related Socio-Economic Data Sheets for Countries of Social Commission for Western Asia as Assessed in 1996 (Beirut: ESCWA, 1997).
The region’s economic dependency — the ratio of the economically inactive to economically active population — is the highest in the world. Because of its young age structure and low level of female labor force participation, the proportion of the population that is economically active is lower in MENA than in all other regions. According to the International Labour Organization (ILO), the only countries with a dependency ratio of two or higher (an average of two or more persons not economically active per one economically active person) are found in the MENA region.2
Commitment to political stability, investment in health and human resources, and sound economic policies can turn the population challenges of MENA to “demographic bonuses.” A demographic bonus may occur, for example, when a large young population is healthy, educated, trained, and ready to be absorbed in a market economy and to contribute to the national economy. Unfortunately, MENA countries are currently more likely to experience “brain drain,” as large flows of educated people leave the region for Europe, North America, and other parts of the world.
Many governments struggle to provide for the basic needs of their growing populations. MENA’s unemployment rate is the highest in the world. According to one analysis, between 1996 and 2010, MENA economies will need to create half again as many additional jobs as those that existed in 1996 in order to prevent the region’s unemployment rate from increasing above its mid-1990s’ rate of about 14 percent — assuming the proportion of working-age population who enter the labor market remains unchanged.3 The Egyptian economy, for example, needs to create an additional 500,000 new jobs each year to absorb new entrants into its job market. Even some of the oil-rich countries in the Gulf, such as Saudi Arabia, which have traditionally had no unemployment, are faced with youth unemployment.
Unemployment is highest among young people and women. In Jordan in 1997, three-quarters of the unemployed were 15 to 29 years of age, and the female unemployment rate was twice as high as that of men.4 Women in MENA face the highest rate of unemployment in the world. According to the ILO, the largest gender gaps in unemployment are found in MENA. Unemployment rates in Egypt were reported to be 24 percent for women in 1995, compared to 7 percent for men.5
To prepare its growing working-age population for the era of economic globalization, MENA requires a much greater investment in human resources. Despite governments’ efforts in the area of education, the number of illiterate adults continues to increase in some countries. In Egypt, between 1980 and 1995, the literacy rate among the population age 15 years and older increased from 40 percent to 50 percent, but the total number of illiterate Egyptians still grew from 16 million to 19 million. Morocco’s illiterate population grew from 8 million in 1980 to 9.5 million in 1995, despite the increase in its literacy rate from 29 percent to 44 percent.6 Two-thirds of MENA’s illiterate adults are women.
Managing rapidly growing urban populations in the face of housing shortages and inadequate infrastructure is also becoming more of a challenge. The populations of cities are growing faster than the populations of the countries as a whole, as population growth in the rural areas feeds a pool of potential rural-to-urban migrants. Currently, Cairo (10.6 million), Istanbul (9.6 million), and Tehran (7.2 million) are ranked 19th, 22nd, and 28th in the world, respectively. By 2015, Cairo (13.8 million) and Istanbul (12.5 million) are projected to rank 16th and 17th.7
Rapid population growth threatens MENA’s sustainable development, as the region is faced with the most severe water shortage of any region in the world. While it is home to 6.3 percent of the world’s population, MENA holds only 1.4 percent of the world’s accessible fresh water. Between 1970 and 2001, population growth caused the available renewable fresh water resources per person in MENA to drop by more than half: from 3,300 to 1,500 cubic meters per person per year. The per capita fresh water resources available are projected to decline to around 1,000 cubic meters by 2025, the internationally recognized threshold for water scarcity. Today, much of the region is already below the international standard, since nearly 80 percent of available fresh water in the region is found in Iran, Iraq, Syria, and Turkey. In countries such as Israel, Jordan, Kuwait, and Saudi Arabia, the national average is below 200 cubic meters per person per year.8
Peace and political stability in the region are necessary for governments to address some of their population challenges, particularly those of refugees. MENA, home to more than 6 million refugees, has the largest refugee population in the world. Iran has the largest number of refugees living in its territory. Palestinian refugees are the largest and oldest refugee population in the world.9
In addition to a commitment to peace and political stability, sound environmental, social, and economic policies are needed to address these and a variety of other population-related challenges, such as labor migration and environmental degradation. Different policies ranging from labor and trade laws and regulations to those related to raising the status of women and protecting the environment all need to take into account the population factor. To have a better understanding of the population factor, future MENA policy briefs will examine different population issues, highlighting regional and national approaches, success stories, and lessons learned.
The following section briefly highlights how the international community is addressing population at a global level and what MENA’s experience has been.
The United Nations (UN) held its first meetings on global population in 1954 and 1965, warning that rapid population growth could exacerbate poverty and hinder development in countries with limited resources. In 1969, the UN created the United Nations Population Fund (UNFPA), whose mission included the promotion of national family planning programs. From this time onward “population programs” and “family planning programs” became almost synonymous. Egypt, Iran, and Turkey were among the first less developed countries to officially support family planning. These governments set up family planning programs in the 1960s to improve health and lower population growth as part of their national development plans.10
On the other hand, there were countries such as Algeria that did not see a need for organized family planning programs as part of their national development plans. At the 1974 UN World Population Conference in Bucharest, Algeria was among the countries leading the opposition to family planning programs on the grounds that they were an imperialist conspiracy aimed at limiting the population of the developing world. This group of countries believed that a national family planning program could not play a part in socioeconomic development, and only socioeconomic development was capable of creating the necessary environment for fertility to decline. Later, however, the Algerian government realized that development alone would not be sufficient to lower fertility and reversed its policy. In 1983, Algeria adopted a population policy that promoted family planning as part of its national development plan.
Iran reversed its official position on family planning twice since the 1960s. Soon after its 1979 Islamic revolution, Iran dismantled the previous regime’s population program because it was viewed as pro-West. After the Iran-Iraq war ended in 1988, the government of Iran turned its focus to the reconstruction of its war-ravaged country. It saw rapid population growth as a major obstacle to the economic development of the country and began to implement one of the most successful population programs in the less developed world.
All governments attending the Second Amman Population Conference in 1993, the regional preparatory conference for the UN’s International Conference on Population and Development (ICPD) held in Cairo in 1994, recognized family planning as a health and human rights measure that was sanctioned in Islam. Currently, no government in the region restricts married couples’ access to family planning information and services. Most support the provision of family planning information and services, directly or indirectly, as part of their primary health care services. A number of countries, such as Algeria, Egypt, Iran, Jordan, and Turkey, have adopted explicit policies to lower fertility and have implemented national information and education campaigns to encourage smaller families.
The 1994 Cairo conference was a landmark in the series of UN population conference because it emphasized individual needs and well-being beyond family planning-including the need for comprehensive reproductive health care and improvements in the status of women. Reproductive health, defined for the first time in an international policy document, includes ensuring healthy and safe childbearing, preventing sexually transmitted infections (including HIV/AIDS), and addressing other factors that contribute to poor health, such as sexual trafficking and violence against women. Major reproductive health issues facing the MENA region are high maternal mortality (particularly in Yemen, Morocco, Egypt, and Iraq) and the increasing prevalence of sexually transmitted infections and HIV/AIDS. High fertility, slowing fertility decline, early marriage, and high teenage fertility are major reproductive health concerns in a number of MENA countries. The practice of female genital cutting, though unknown in some areas outside Egypt and Yemen, is a major reproductive health issue that has brought national and international human rights, health, and women organizations together to call for its eradication.11
The Cairo Programme of Action calls on governmental and nongovernmental organizations and international development agencies to increase their support for and investments in reproductive health, girls’ education, and raising the status of women (see Box 1, below). All governments participating in the Cairo conference endorsed its Programme of Action. For Muslim countries, including those in MENA, the endorsement generally came with the reservation that they would interpret and adopt its recommendations in accordance with Islam-a position needed for the delegations to take the recommendations back home for implementation. The Programme of Action touched on issues such as youth sexuality and empowerment of women, which are culturally sensitive in some Muslim countries.
The Cairo Programme of Action acknowledges that the implementation of its recommendations “is the sovereign right of each country, consistent with national laws and development priorities, with full respect for the various religious and ethical values and cultural background of its people, and in conformity with universally recognized international human rights.”12 While building on the experiences of countries in other regions that have addressed their population challenges, MENA countries are considering how to achieve socially equitable, sustainable development in their own cultural and social context (see Box 2, see below).
Other UN international conferences in the 1990s focused on related aspects of human development: World Summit for Children (New York, 1990), Conference on Environment and Development (Rio de Janeiro, 1992), World Conference on Human Rights (Vienna, 1993), World Summit for Social Development (Copenhagen, 1995), Fourth World Conference on Women (Beijing, 1995), and Conference on Human Settlements, known as Habitat II (Istanbul, 1996). The Cairo agenda and its emphasis on meeting reproductive health needs and raising women’s status build on the outcomes of the UN conferences that preceded it, and they are reaffirmed in those that followed it. The recommendations resulting from these conferences provide a framework for achieving socially equitable, sustainable development that each country can adapt to their own circumstances.
This overview of population trends and challenges in the MENA region is the first in a series of policy briefs from the Population Reference Bureau that analyze population, environment, reproductive health, and development linkages within the framework of the Cairo Programme of Action and the cultural contexts of population groups in the region. Future briefs on MENA will cover specific population-related topics or country case studies.
Thanks are due to Ismail Sirageldin and Tom Merrick who reviewed the draft and offered useful comments. This work has been funded by the Ford Foundation.
Box 1:
The Cairo Programme of Action Set a Number of Goals
The UN’s International Conference on Population and Development (ICPD), held in Cairo in 1994, provided an opportunity for MENA countries, as well as other countries around the world, to examine their population challenges and to discuss possible solutions. The ICPD’s Programme of Action, adopted by 179 participating countries, provides a comprehensive framework for slowing population growth and improving people’s lives. Focusing on human development, the document calls for a wide range of investments to improve health, education, and rights — particularly for women and girls — and to provide family planning services in the context of comprehensive reproductive health care.
ICPD set the following quantifiable goals for 2015:
Source: United Nations Population Fund (UNFPA), “Programme of Action of the International Conference on Population and Development” (New York: UNFPA, 1994): paragraphs 7.16, 8.16, 8.21, 8.5, and 11.8.
Box 2:
Cairo in Action
Since the Cairo conference, many countries have taken concrete policy actions toward the goal of providing universal access to reproductive health care. In some cases, these actions included developing comprehensive national reproductive policies; in others, governments redesigned aspects of existing family planning or other health programs to address reproductive health. The following are examples from MENA:
Sources: Country presentations at the UN General Assembly for the Overall Review and Appraisal of the Implementation of the ICPD Programme of Action, New York, July 1, 1999; and statement by Dr. Nafis Sadik, executive director, UNFPA, at the luncheon for the Congressional Women’s Caucus, Washington, DC, July 20, 1999.
 ">
">