Beth Jarosz
Senior Program Director

Vaccines are one of the simplest, most cost-effective tools to improve public health. Vaccine-preventable diseases can lead to illness, disfigurement, and disability, and remain a substantial cause of death for young children. Globally, immunization rates improved dramatically in the 1980s and 1990s, but progress has stalled in recent years.
Each year, about one in five children who dies before his or her fifth birthday, dies from a vaccine-preventable disease. Measles alone kills more children worldwide each year than HIV/AIDS, Sudden Infant Death Syndrome, traffic accidents, or drowning.1
Vaccines protect individuals, and with high rates of coverage, can also provide “herd” immunity: When many children within a community are immunized, infectious diseases do not spread to those who cannot be immunized—very young infants or those for whom vaccines are not recommended due to certain illnesses, allergies, or immune system problems. Protecting children’s health through vaccinations benefits parents as well, because they can save money on health care costs later and also miss fewer days of work to care for sick children, making them more economically productive.
The U.S. Centers for Disease Control and Prevention (CDC) has identified 15 vaccine-preventable childhood diseases, ranging from influenza to polio.2 This article focuses on four vaccine-preventable diseases—diphtheria, measles, pertussis (whooping cough), and tetanus—that caused an estimated 218,400 deaths worldwide in 2013.3 Of those deaths, more than three-quarters were to children under age 5. These deaths could have been prevented if children had been fully vaccinated.
Diphtheria, tetanus, and pertussis are addressed by a combination vaccine, DTP.4 While countries have a wide range of immunization schedules, the World Health Organization (WHO) recommends a minimum of three doses of DTP vaccine (DTP3).5
Measles vaccination is often added with other diseases in a combination vaccine, but the combinations vary by country. Measles-containing vaccines (MCV) are most effective when at least two doses are administered.6
The good news is that immunization coverage has increased globally and vaccine-preventable child deaths and illnesses have declined since the 1980s.
This substantial improvement over the past few decades can be credited to increased vaccination rates, but rapid progress made during the 1980s and 1990s slowed and then stalled in recent years (see figure).
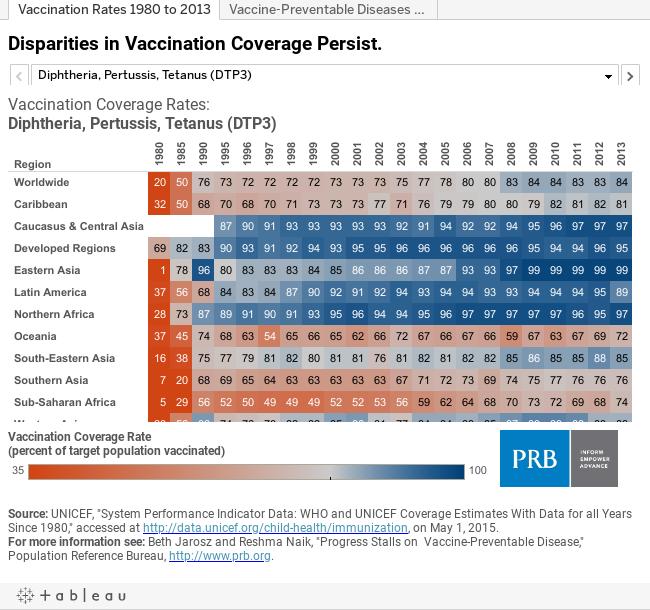
For example, coverage with a third DTP vaccination increased dramatically from 20 percent worldwide in 1980 to 76 percent in 1990. The rate dipped slightly in 2000 before rising to 84 percent in 2009, but no improvement in DTP coverage has been made in the past five years.
Worldwide, coverage rates for a single dose of MCV have also hovered around 84 percent for the past five years. The two-dose recommended MCV vaccination continues to show steady improvement, but in 2013 only 53 percent of the target population had received a second dose of measles vaccine.7
As a result of stalled progress on immunization, vaccine-preventable diseases remain a global problem, and in some areas are actually resurging.
In 2013, four vaccine-preventable diseases (measles, diphtheria, tetanus, and pertussis) resulted in nearly half a million illnesses and more than 200,000 deaths worldwide. Adding mumps and rubella brings the total count of vaccine-preventable illnesses to well over 1 million cases in 2013 (516,000 cases of mumps and 101,000 cases of rubella).
In the United States, as in other countries, outbreaks of measles and pertussis have made headlines in recent years, including the 20-state outbreak of measles in 2015 linked to California’s Disneyland amusement park. Moreover, California alone had more than 9,000 cases of pertussis in 2010 and more than 11,000 cases in 2014.8
The proportion of vaccinated children varies across world regions.9 In much of the world, those who are underserved by vaccines tend to be poor or live in strife-torn, remote, or deprived urban areas.
For DTP3 vaccinations, coverage ranges from 72 percent in Oceania to 99 percent in Eastern Asia. Coverage with a single dose of MCV is similar, ranging from 73 percent to 99 percent across regions. While the global goal for both vaccines is at least 90 percent coverage worldwide, the global average for both vaccinations remains at 84 percent, and in many regions one in four children remain unvaccinated.
Second-dose MCV is a new WHO recommendation and not yet widely adopted. As of 2013 (the first year of reporting) in some countries, mostly in Africa and the Middle East, no children had received MCV2. Other countries are doing much better, with as many as 99 percent of children having received a second dose of MCV. Globally, just over half of all children have received both doses of this critical measles-containing vaccine.10
In 2013, gaps in vaccination coverage meant that nearly 22 million infants globally did not receive all three doses of DTP. More than half did not receive the first dose and the rest started, but did not complete the series. Nearly 70 percent of these incompletely vaccinated children live in only 10 countries. Half live in three countries—India, Nigeria, and Pakistan.11
Disparities within countries are also important. In 2013, two-thirds of countries achieved the global target of 90 percent DTP3 coverage. But national rates only tell part of the story.In the same year, more than 70 percent of countries failed to achieve 80 percent DTP3 coverage in every district or equivalent administrative unit.
In the United States, as in other countries, vaccination coverage varies by geographic location. In 17 states MCV1 coverage rates (usually addressed by the measles, mumps, rubella, or MMR, vaccine) are below 90 percent. The highest rate of MCV coverage is in New Hampshire (96 percent) and the lowest is in Colorado (86 percent). Rates for DTP coverage vary even more widely. Coverage with at least four doses of DTP (the level reported by state in the United States) ranges from 74 percent (Arkansas) to 93 percent (Massachusetts). Only five states exceed 90 percent DTP4 coverage.12
These local variations exist, in large part, because rules regarding immunizations and immunization exemptions vary by state. All states have rules that require vaccination before enrolling in school, preschool, or daycare, but some state regulations are more stringent than others.
Within states there is also unequal coverage. In California, for example, the proportion of kindergarten students in 2015 who received all state-required immunization ranges from 100 percent (Sierra County) to 73 percent (Nevada County) and school district coverage rates vary even more widely, and in Colorado, another state which has broad immunization exemption policies, more than half of children in some schools have immunization exemptions.13
Low rates of vaccination, and high rates of vaccination exemptions, tend to be geographically clustered. As a result, vaccine-preventable disease outbreaks can, and do, occur where unvaccinated persons cluster in schools and communities, even within countries with high overall vaccination coverage. And some diseases considered to be eliminated can reappear. In 2014, for example, the United States saw a record 668 measles cases across 27 states, despite the fact that measles elimination was documented in the United States in 2000.
In another article, we explore the reasons for gaps in global vaccination coverage and potential solutions.