Today's Research on Aging: Rising Obesity in an Aging America
U.S. obesity is slowing gains in life expectancy and widening racial health disparities. New research examines the health impact and social consequences of obesity to inform intervention and prevention strategies.

Obesity rates have risen dramatically in recent years, nearly doubling among older U.S. adults to include two in every five Americans ages 65 and older. For individuals, prolonged obesity increases the risk of chronic disease, disability, and early death, along with high health care costs and greater odds of needing nursing home care.
Addressing the obesity epidemic will require attention to both individual behaviors and contextual factors such as socioeconomic disparities and burdens of discrimination. These behaviors and factors contribute to differences in obesity prevalence across populations.
This issue of Today’s Research on Aging examines recently published work of National Institute on Aging-supported researchers probing the health impact and social consequences of obesity. Understanding these dynamics can inform more effective intervention and prevention strategies and enable policymakers and health care administrators to plan for the challenges ahead.
Obesity Rates Have Increased Sharply Among Older U.S. Adults
Obesity prevalence among older Americans is increasing at an alarming rate. In a single generation—between 1988-1994 and 2015-2018—the share of U.S. adults ages 65 and older with obesity nearly doubled, increasing from 22% to 40% (see Figure 1).1 During the same period, the share of older men with obesity rose from 20% to 38%, while obesity prevalence among older women increased from 24% to 42%. The U.S. Centers for Disease Control and Prevention (CDC) defines obesity as having a body mass index (BMI) of 30 or higher. BMI is an indirect measure of body fat that does not distinguish among excess fat, muscle, or bone mass, notes the CDC.2 BMI is not a diagnostic tool but provides a useful starting point to identify potential health risks. The CDC recommends BMI be used to “track weight status in populations” and “as a screening tool to identify potential weight problems in individuals.”
FIGURE 1. Obesity Rates Among Older Adults in the United States Have Nearly Doubled in a Generation
U.S. Adults Ages 65 and Older With Obesity, by Sex and Age Group, Selected Years, 1988-2018

Note: Data are based on measured height and weight. Obese is defined as having a body mass index (BMI) of 30 kilograms per meter squared or greater.
Source: National Center for Health Statistics, National Health and Nutrition Examination Survey.
During the three-decade period from 1998 to 2018, the rate of increase was most dramatic among the “young old” (ages 65 to 74)—the share who were obese increased from 24% to 42% for men and from 27% to 46% for women. Obesity rates also increased sharply among men and women ages 75 and older, although their rates were slightly lower.
High obesity rates among working-age adults suggest obesity prevalence among older Americans could continue to rise in the coming years. In 2017-2018, nearly 45% of adults ages 40 to 59 were classified as obese—more than any other age group.3
Obesity Raises Risks of Chronic Disease, Increases Disability, and Shortens Lives
Older people with obesity face a higher risk of chronic illness such as cardiovascular disease and diabetes, functional limitations, and shorter lives than their peers without obesity. During the coronavirus pandemic, people with obesity also have an elevated risk of hospitalization and death from COVID-19, with severity rising dramatically with higher BMI, the CDC reports.4 New studies are examining the impact of U.S. obesity trends on older Americans’ life expectancy, health, and disability.
The rise in obesity appears to be slowing improvements in U.S mortality rates and life expectancy, leaving the United States trailing many other affluent countries that have lower obesity levels (see Figure 2).5 Samuel Preston, Yana C. Vierboom, and Andrew Stokes estimate that rising obesity slowed the annual U.S. mortality decline by one-half of a percentage point, a large amount in this context. Rising BMI between 1988 and 2011 reduced gains in life expectancy at age 40 by nearly one year, representing about 186,000 excess deaths in 2011, they report.
“The headwinds posed by increasing levels of BMI have prevented the United States from enjoying the full benefits of reductions in smoking and advances in medical technology,” they write. “Continued gains in BMI would threaten future gains in life expectancy as well.”
FIGURE 2. Obesity May Explain Why Mortality Improvements in the United States Lag Behind Other Wealthy Countries
Annual Rates of Mortality Decline Among Adults Ages 40 to 84 in Selected OECD Countries, 1988-2011

Note: OECD refers to the Organisation for Economic Cooperation and Development.
Source: Samuel H. Preston, Yana Vierboom, and Andrew Stokes, “The Role of Obesity in Exceptionally Slow U.S. Mortality Improvement,” PNAS 115, no. 5 (2018).
Obesity may be slowing life expectancy gains by accelerating biological aging, particularly among U.S. women, report Morgan E. Levine and Eileen M. Crimmins.6 Biological aging occurs more rapidly in some individuals than others, contributing to earlier onset of chronic disease, disability, and mortality. Using health and multiple biomarker data from more than 21,500 Americans, the researchers calculated the differences in biological age relative to chronological age between 1988 and 2010 among those with and without obesity in relation to smoking. Among nonsmokers, people who were overweight aged more than one year faster on average, and people with obesity aged more than two years faster compared with their peers with a BMI under 25.
If recent increases in obesity and overweight (BMI 25.0 to 29.9) had not occurred, Levine and Crimmins estimate that young adults in their 20s and 30s would have aged 38% to 72% more slowly during the period. They argue that if obesity speeds up the timing of age-related disease and disability, medical costs will rise, and more people will live more of their lives in poor health. In addition, today’s young adults may not experience the same gains in life expectancy that earlier generations saw.
Preventing obesity earlier in life may be especially important to preserve good health in later years. Kaitlyn M. Berry and colleagues found that BMI at age 54 was more strongly associated with late-life mortality than BMI at older ages.7 Knowing older people’s weight at midlife and how their weight has changed may be more important in assessing their late-life mortality risk than their current weight because some chronic diseases cause people to lose weight at older ages, they argue.
High BMI early in life also contributes to the risk of developing a disability—that is, difficulty with everyday activities such as bathing, preparing meals, or doing heavy housework— separate from BMI in later life. Tarlise N. Townsend and Neil K. Mehta used data from the Panel Study of Income Dynamics to study the relationship between individuals’ BMI in 1986 and disability incidence in 2003-2015. They found that earlier-life BMI accounted for about one-fifth of incident disability among adults ages 33 to 69.8 Obesity, along with smoking, may be contributing to stagnating disability levels after decades of improvement, they suggest.
The increase in obesity may also be reflected in rising levels of chronic pain among middle-age and older adults. Using data from 1992 to 2016 from the U.S. Health and Retirement Study (HRS), Andrew Stokes and colleagues found that increases in BMI over the previous 24 years may account for a significant share of the rise in severe and/or limiting pain, up to about one-third for women and one-fifth for men.9 Debilitating pain is related to suicide, opioid use, and death, and thus may represent another “important pathway linking obesity to mortality trends,” they argue.
Obesity also contributes to heart disease, but despite rising obesity rates, both American men and women ages 50 and older cut their risk of heart disease and stroke between 1990 and 2010, Jung Ki Kim, Jennifer Ailshire, and Crimmins show.10 What explains this dynamic? The researchers suggest the reason may be declining rates of smoking and wide use of effective prescription medications for reducing high blood pressure and cholesterol levels.
Another study suggests that medical treatment for both cardiovascular diseases and diabetes may be slightly lengthening lives and reducing disability among all older Americans, including those with obesity, Yuan S. Zhang, Yasuhiko Saito, and Crimmins find.11 In 2010-2014, Americans ages 70 and older with and without obesity could expect to live a somewhat smaller portion of their remaining life with a disability related to activities of daily living (that is, difficulty bathing, dressing, eating, using the toilet, or getting in and out of bed) compared with those in 1993-1998 (see Figure 3).
The researchers point to two other reasons that may explain these small disability declines:
- The older population is more educated than the earlier generation, and higher levels of education are linked to better health and greater longevity.
- Older adults with physical limitations may be relying more on home modifications (such as grab bars and chair lifts) and assistive devices (such as walkers) to continue to function independently.
Yet, the researchers emphasize that older people with obesity continue to live shorter lives and spend a greater portion of their last years disabled than people without obesity. (Also see box.) “The increasing prevalence of severe obesity and the growing number of older persons may result in substantial additional health care needs and costs,” they warn. “Continued effort to improve cardiovascular health is required to control the burden of obesity in later life in an era of rising obesity,” they argue.
FIGURE 3. People With Obesity Spend More of Their Later Years With a Disability Compared With Those Who Are Not Obese
Percent of Remaining Life Disabled Among Men and Women at Age 70, by Level of Obesity, 1993-1998 and 2010-2014
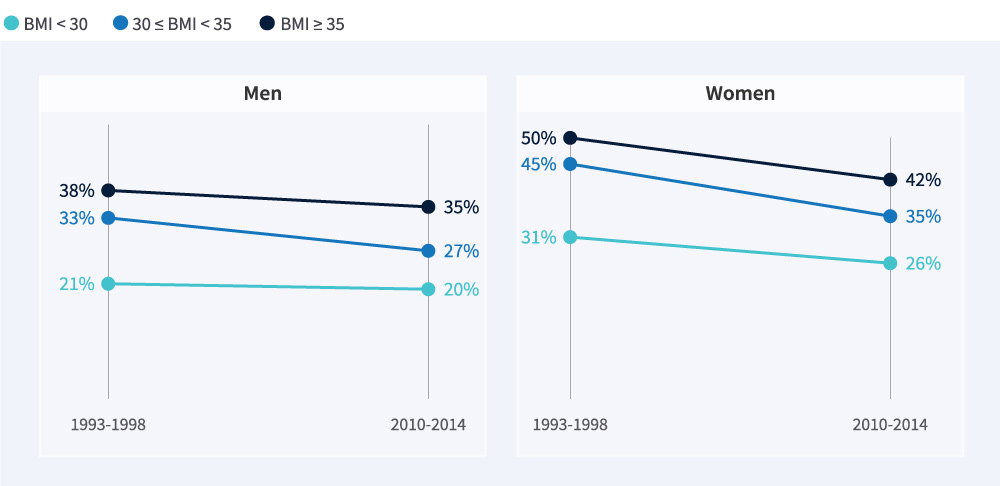
Source: Yuan S. Zhang, Yasuhiko Saito, and Eileen M. Crimmins, “Changing Impact of Obesity on Active Life Expectancy of Older Americans,” Journals of Gerontology, Series A: Biological Sciences and Medical Sciences 74, no. 12 (2019).
Obesity Is Contributing to Racial/Ethnic Health Disparities
As U.S. life expectancy gains have slowed or stagnated, mortality gaps related to race/ethnicity and education level have widened. Obesity appears to play an important role in these gaps. Using HRS data, Peter Hudomiet, Michael D. Hurd, and Susann Rohwedder identified 15 health indicators (including BMI) that together can predict survival to older ages.12 They found most of these indicators had worsened between 1992 and 2016. They also documented greater health inequalities by race/ethnicity and education level in recent years compared with the 1990s. Health decreased more among individuals with lower education levels compared with more educated individuals, and it decreased more among Black and Hispanic adults than non-Hispanic white adults, they report. Inequalities in class 2 obesity (BMI 35 or higher) at ages 55 to 59 rose substantially (see Figure 4).
The observed increases in midlife health inequalities “will likely translate into further increases in mortality inequalities over the next decades,” they write, arguing that policies that improve the health of individuals with low incomes and education levels “would likely help reverse the adverse trends in mortality.”
FIGURE 4. Since the 1990s, Obesity Rose Most Sharply Among Older Black and Hispanic Americans
Class 2 Obesity Rates Among Adults Ages 55-59, by Sex, Race/Ethnicity, and Year

Note: Class 2 obesity is BMI 35 or higher. The categories White, Black, and Other Race are non-Hispanic.
Source: Peter Hudomiet, Michael D. Hurd, and Susann Rohwedder, “Trends in Health in Midlife and Late Life,” Journal of Human Capital 16, no. 1 (2022).
The Black-white disparity in premature death may be explained by the way obesity, smoking, and education levels interact to impact health, Irma T. Elo, Neil Mehta, and Samuel Preston show.13 Using data on Americans ages 40 to 79 from the National Health and Nutrition Examination Survey (NHANES), they show that key risk factors for premature death are obesity among Black women and smoking among Black men, accounting for 30% and 17% of the Black-white mortality gap, respectively. Lower educational levels explain an additional one-fifth of the Black-white mortality gap among Black men and one-quarter of the gap among Black women. Low educational attainment is associated not only with smoking and obesity but also with lifelong economic hardship, inferior access to health care, and a range of other factors pertinent to health, the researchers explain. Smoking, for instance, may be a way of coping with stressful life conditions, they suggest.
Racial/ethnic and educational disparities in BMI are larger in recent generations compared with earlier generations, researchers mainly affiliated with the Carolina Population Center, University of North Carolina (UNC) at Chapel Hill show.14 They analyzed changes in BMI during the aging process by combining data from four national longitudinal surveys totaling about 65,000 respondents grouped into five-year birth cohorts spanning 1905 to 1984. Each successive cohort had a higher average BMI and a steeper rise in BMI with age, compared with the prior cohort. Not only were racial and educational disparities in BMI larger for more recent cohorts than for previous cohorts, BMI-related disparities emerged early in life and were more substantial for women than men.
“Our results reveal that socioeconomic inequality does not fully account for racial/ethnic disparities in BMI, especially when further stratified by gender,” the UNC researchers report. “Burdens of discrimination and differential access to health-promoting resources may accelerate biological processes of aging or trigger less health-promoting coping behaviors,” they assert.
Racism-related stress is also associated with an increased obesity risk: Black men who reported any major discrimination—including being unfairly fired or not hired, mistreated or abused by police, or prevented from moving into a neighborhood—were more likely to be obese than Black men who did not report any such major discrimination, Roland Thorpe Jr. and colleagues documented.15 Their analysis took into account age, income, education, health conditions, other major stressors, and physical activity. By contrast, Black men who reported experiencing everyday discrimination—such as being followed in stores or treated with less respect—had the same obesity rate as their peers who did not report any type of discrimination.
“These findings provide evidence that the consequences of major discrimination extend to obesity in African-American men,” the researchers write. They call for further study to explore “how psycho-social stressors, namely discrimination, can impact obesity and its persistence over time.”
BOX
Obesity in Midlife Is Linked to Increased Risk of Dementia Obesity’s role in dementia risk has puzzled researchers: Some studies show that obesity in midlife (between ages 40 and 60) is linked to lower cognitive function and increased dementia risk in old age. But obesity after age 65 appears to provide some protection from dementia, while being underweight at older ages raises dementia risk, reports Kenneth Langa and colleagues based on nationally representative U.S. Health and Retirement Study (HRS) data. One theory is that being overweight or obese at older ages might provide buffering reserves of muscle and fat that slow the progression of chronic disease, while unintentional weight loss may be an early sign of dementia onset. Another theory suggests that the link between being underweight and developing dementia is so strong that people with obesity appear to be protected from dementia.Ida Karlsson and colleagues also analyzed a related set of HRS data and noted the link between being underweight and having dementia. But they also find a strong connection between higher BMI and declining cognitive abilities throughout both midlife and late life, especially among men and individuals with genes that predispose them to a low BMI. Similarly, a recent study based on data from the English Longitudinal Study of Ageing shows that overweight or obese older adults were more likely than their peers to develop dementia 11 years later. Women face a higher dementia risk than men related to their having central obesity (high waist circumference). In addition, the study finds that the association between obesity and dementia is independent of whether a person was a smoker, had hypertension or diabetes, or carried the APOE ε4 gene, a genetic risk factor for Alzheimer’s disease and related dementias.

Obesity Begins to Shape Old-Age Health During Young Adulthood
A complex set of interrelated factors play a role in obesity, including diet, physical activity, genetics, stress, and an individual’s environment—which can include everything from lack of parks to food advertising. Researchers are trying to understand how and when these factors begin to create a trajectory for increased health risks later in life.
Inflammation related to obesity may speed up biological aging early in life, setting the stage for chronic diseases later in life. Steven W. Cole and colleagues found that obesity in young adulthood may trigger the expression of inflammation-related genes in young adults that contribute to chronic illness and premature death at older ages.16 Daniel Parker and colleagues show that beginning as early as their 30s, young adults with high BMI experience age-related changes in immune and metabolic biomarkers known to be associated with chronic disease, disability, and premature death in older adults.17
Another recent study linked high BMI early in life with increased cardiovascular disease risk due to chronic low-grade systemic inflammation: High BMI at age 3 sustained through young adulthood was related to signs of cardiovascular disease (endothelial dysfunction, a type of nonobstructive coronary artery disease) as early as age 38.18 In addition, among adolescents with high BMI, the stress of childhood trauma and depression combine to amplify obesity-related inflammation, heightening health risks, Jessica Chiang and colleagues found.19
Both nature and nurture—that is, an individual’s genes and the environment in which they live, play, and work—contribute to obesity. But timing is also important: Gene variants known to both regulate body fat and increase the risk of dementia behave differently in young adults versus older individuals, Alexander M. Kulminski and colleagues found.20 Another study that examined twin pairs on four continents over 60 years shows that genes have a strong influence on BMI, regardless of the obesity level in the population, particularly in young adulthood.21 As the twins aged, the role of genetics in influencing BMI shrank and environmental factors played a greater role in later life.
Sleep patterns may be among the environmental factors that shape obesity. Michael J. Parsons and colleagues found that individuals with a greater prolonged difference in sleep between free days and workdays are more likely to be obese and suffer from obesity-related disease than those with little to no difference between these timings.22 As little as sleeping an additional two hours on days off of work can increase the risk of an elevated BMI and biomarkers for inflammation and diabetes, they warn.
The Financial and Societal Challenges of Obesity in Aging Americans
Not only do Americans with obesity face a high risk of chronic conditions and disability at older ages but they also tend to use more health care, which raises costs for both individuals and governments.23
But the costs of obesity to individuals are more than monetary. HRS data show that older adults with obesity are less likely to get the help they need with everyday activities and more likely to move into a residential care facility than their peers. Because they are overweight, getting them in and out of bed is physically demanding, making it more difficult to find help at home from paid caregivers or family and friends, explain Claire K. Ankuda and colleagues.24
Older adults with obesity also have higher odds of poor-quality end-of-life care. Analysis of HRS data shows they are less likely to use home hospice or die at home (as most people prefer), and are more likely to incur higher Medicare expenditures in their last six months of life than their counterparts without obesity.25 John A. Harris and colleagues recommend policymakers increase Medicare reimbursement rates for home care for people with obesity and make specialized medical equipment such as lifts more widely available.
On a national level, Hudomiet, Hurd, and Rohwedder forecast a growing longevity gap between those with high and low Social Security wealth, based on analysis of mortality trends and health risks (including obesity) among successive groups of 54-to-60-year-olds born between 1934 and 1959.26 They predict a six- to eight-year gap in survival between those with high and low Social Security wealth among the oldest group, who averaged age 84 in the study. Among Baby Boomers born in the late 1950s, they predict a mortality gap of 14 or 15 years between those with high and low Social Security wealth.
“These changes will exacerbate the already substantial financial challenges of Social Security and Medicare,” they warn.
Addressing health disparities between different socioeconomic groups could help reverse this trend. But policies that lower levels of central obesity (high waist circumference) may widen health disparities between highly educated adults and those with low education levels because of the role this type of obesity plays in premature death, Iliya Gutin found.27 He shows that premature deaths attributed to central obesity (particularly coronary heart disease, heart attack, and stroke) make up a far larger share of deaths (30% to 70%) among college-educated adults than their counterparts with less education (10% or less). “Central obesity [is] a key risk among highly educated adults, but only one of many encountered by those with less education,” he writes.
To curb obesity and improve health, target ultra-processed foods, research teams affiliated with the University of North Carolina and RAND advocate.28 Mounting evidence links increased consumption of ultra-processed foods (including high-sugar beverages) to an increase in the risk of obesity and noncommunicable diseases such as diabetes, hypertension, and cardiovascular diseases. Successful policies to target these risks could reduce the availability of unhealthy foods; impose levies on manufacturers that produce foods containing an unhealthy number of calories, excessive sugar, and other harmful ingredients; mandate warning labels that inform consumers about the contents of the products they purchase; shield children from junk food marketing; and motivate manufacturers to reformulate food and drink products to make them healthier, the researchers report.
If Americans changed their diets to adhere to nutritional guidelines more closely, the population would be healthier and the nation would see economic benefits, Patricia M. Herman, PhuongGiang Nguyen, and Roland Sturm document.29 Better diets produce small changes in chronic disease prevalence that build up over time: After 30 years, diabetes would drop by more than 11%, heart disease by 7%, and stroke by 10%, their simulation shows. Annual health care savings at year 30 would total $144 billion (in 2019 dollars) with 88,000 fewer deaths; more people would be working for pay and fewer would be disabled, they report.
Policies that improve food security in childhood can also address adult obesity and improve health. Hilary Hoynes, Diane Whitmore Schanzenbach, and Douglas Almond show that having access to food stamps in childhood is linked to a significant reduction in the incidence of metabolic syndrome (obesity, high blood pressure, and diabetes) in adulthood.30
Weight loss is known to provide multiple health benefits, such as improving diabetes control and reducing arthritis pain symptoms. New evidence shows that people considered obese at age 25 can cut their risk of premature death in half if they lose enough weight to be considered overweight—rather than obese—by their mid- to late 40s.31 Wubin Xie and colleagues based their analysis on NHANES data between 1998 and 2015 involving 24,000 U.S. adults. More than 12% of early deaths between young and middle adulthood are related to obesity, they estimate. These findings, they write, provide support for public health policies designed to prevent or reverse obesity, especially among young adults. Weight loss after midlife, however, did not appear to lower an individual’s risk of early death.
Effective Interventions to Address Obesity
Obesity is a leading cause of preventable disease and early death among U.S. older adults. Reversing the obesity epidemic will require a bold, comprehensive plan that reaches people of all ages. The NIA-funded studies summarized in this report provide evidence that supports research and investment in a variety of approaches to prevent and address obesity, including:
- Reduce the availability and consumption of ultra-processed foods and sugary beverages, especially in schools.
- Improve food security, especially among families with children.
- Expand proven school, community, and workplace programs for improving diet and physical activity, particularly those that target youth and young adults.
- Ensure that all adults, especially those with obesity, are screened and treated for risk factors for cardiovascular diseases and diabetes.
- Address the wide range of racial and ethnic disparities related to stress and differences in access to health care, healthy food, and opportunities for physical activity.
To be effective, interventions need to address not only individual behaviors—encouraging healthier diets and exercise—but also contextual factors that contribute to longstanding socioeconomic and health disparities within the U.S. population.
Related Posts
Research Identifies New Strategies to Reduce Undercount of Young Children in U.S. 2020 Census
PRB identifies factors predicting where children under age 5 are more likely to be missed in the 2020 Census and develops a new undercount risk measure for young children.

Lesson Plans on Human Population and Demographic Studies
Find out the answers to these questions and more. The sections listed below explore eight elements of population dynamics.

Report. Population Trends and Challenges in the Middle East and North Africa
(2001) The people of the Middle East and North Africa (MENA) have long played an integral, if sometimes volatile, role in the history of human civilization.
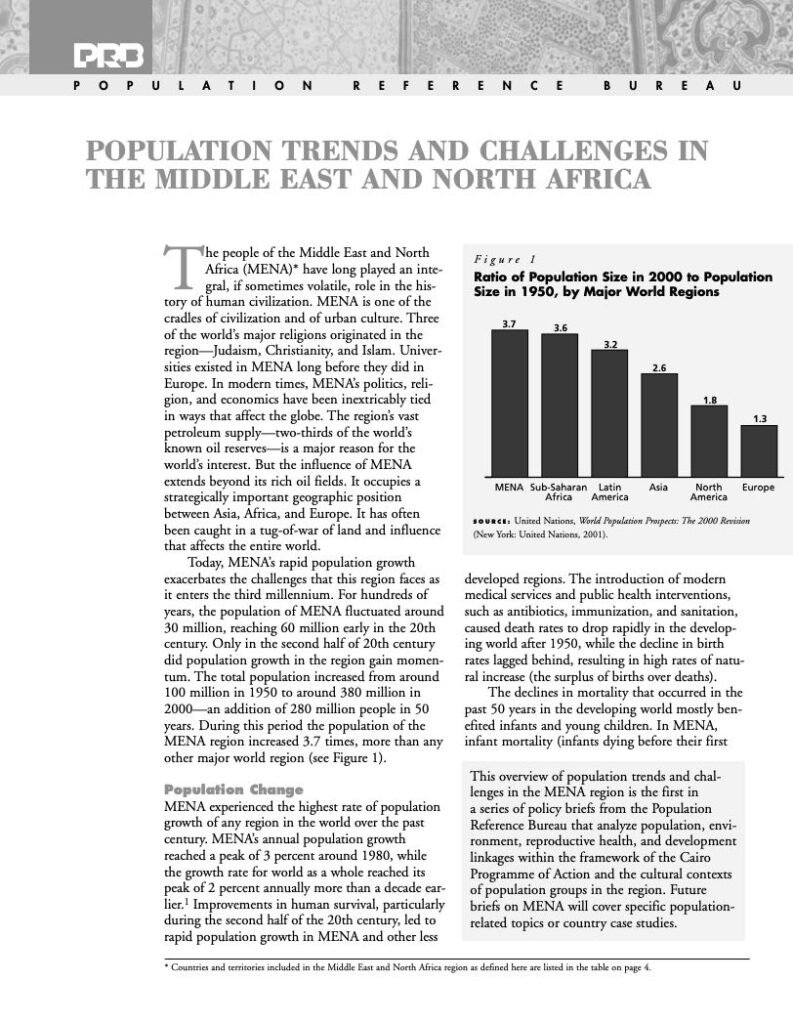
Population Trends and Challenges in the Middle East and North Africa
(2001) The people of the Middle East and North Africa (MENA) have long played an integral, if sometimes volatile, role in the history of human civilization.