Mark Mather
Associate Vice President, U.S. Programs

Dementia is one of the nation’s most expensive old-age health conditions and the most time consuming for family caregivers. As many as 6 million people ages 65 and older live with Alzheimer’s disease in the United States, representing about one in 10 older Americans.1
However, rates of dementia are not uniform across the older population. Those with lower levels of education, the oldest old (people ages 85 and older), women, and racial and ethnic minorities are at greater risk of dementia. The types of living arrangements of people with dementia—whether they live at home, in a residential care setting (such as assisted living), or a nursing facility—also differ depending on the availability of family caregivers and financial resources.
This issue of PRB’s Today’s Research on Aging (Issue 40) summarizes what we know about the characteristics of people with dementia and their caregiving and living arrangements based on studies funded by the National Institute on Aging. Understanding the characteristics of those with dementia can help lawmakers design policies that better meet the needs of this rapidly growing population and their families.
Many conditions and diseases can cause dementia—a set of symptoms that may include memory loss and difficulties with thinking, problem-solving, or language. Alzheimer’s disease is the most common cause, but dementia can also be caused by injuries from impaired blood supply to the brain, often after a stroke. Other types of dementia include Lewy body dementia and frontotemporal disorders.
Alzheimer’s disease and other related dementias are characterized by progressive cognitive decline that interferes with independent functioning. In the National Health and Aging Trends Study (NHATS)—a nationally representative sample of Medicare beneficiaries ages 65 and older—respondents are classified into three categories: those with no dementia, possible (or early stage) dementia, and probable dementia. Participants are classified as having probable dementia if a doctor has told the person that they have dementia or Alzheimer’s disease.
For respondents without a diagnosis, dementia status is determined through a test measuring cognitive functioning, including memory (word recall), orientation (such as knowing the date and year), and executive functioning (drawing a specific time on a clock). In addition, for respondents unable to self-report, proxy respondents (typically a family member) answer the AD8, a series of eight Yes/No questions about the respondent (problems with judgment, reduced interest in hobbies, repeats self, trouble using tools or appliances, forgets correct month/year, trouble handling finances, forgets appointments, daily problems with memory/thinking).2
Cut points (based on standard deviations from the mean) are then used to group study participants into different categories. In the 2011 NHATS, 11% of Medicare beneficiaries ages 65 and older were classified as having probable dementia (10% among the non-nursing home population).3
Clinical guidelines developed by the National Institutes of Health and the Alzheimer’s Association also define three stages of Alzheimer’s disease (the most common type of dementia):
People with advancing dementia (or moderately severe dementia) are more likely to have difficulty with one of three daily living activities (dressing, bathing, or using the toilet) and cognitive difficulties that make it more difficult to manage medications or finances, whereas people with advanced dementia have difficulty with all these functions and more.5
No cure for Alzheimer’s disease currently exists, and no treatments have been proven to prevent its onset or delay its progression, but researchers are studying ways to treat the disease and expand support for people with Alzheimer’s disease and their families.
Prevalence of Probable Dementia Among the U.S. Population Ages 70 and Older, 2015
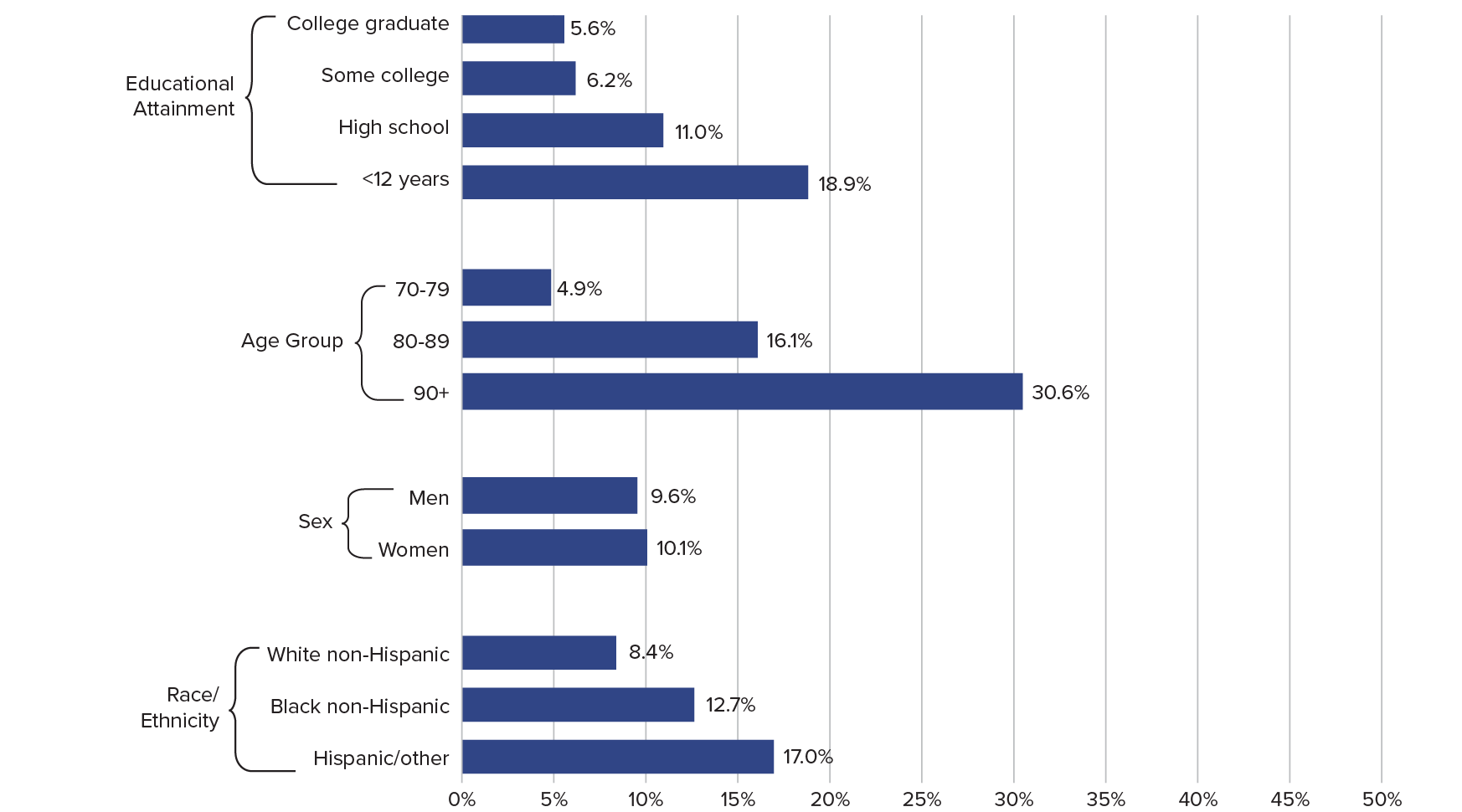
Note: Excludes persons in nursing homes.
Source: Vicki A. Freedman et al., “Short-Term Changes in the Prevalence of Probable Dementia: An Analysis of the 2011–2015 National Health and Aging Trends Study,” Journals of Gerontology, Series B 73 (2018): S48-S56.
Age-Adjusted Death Rates per 100,000 by State, 2017
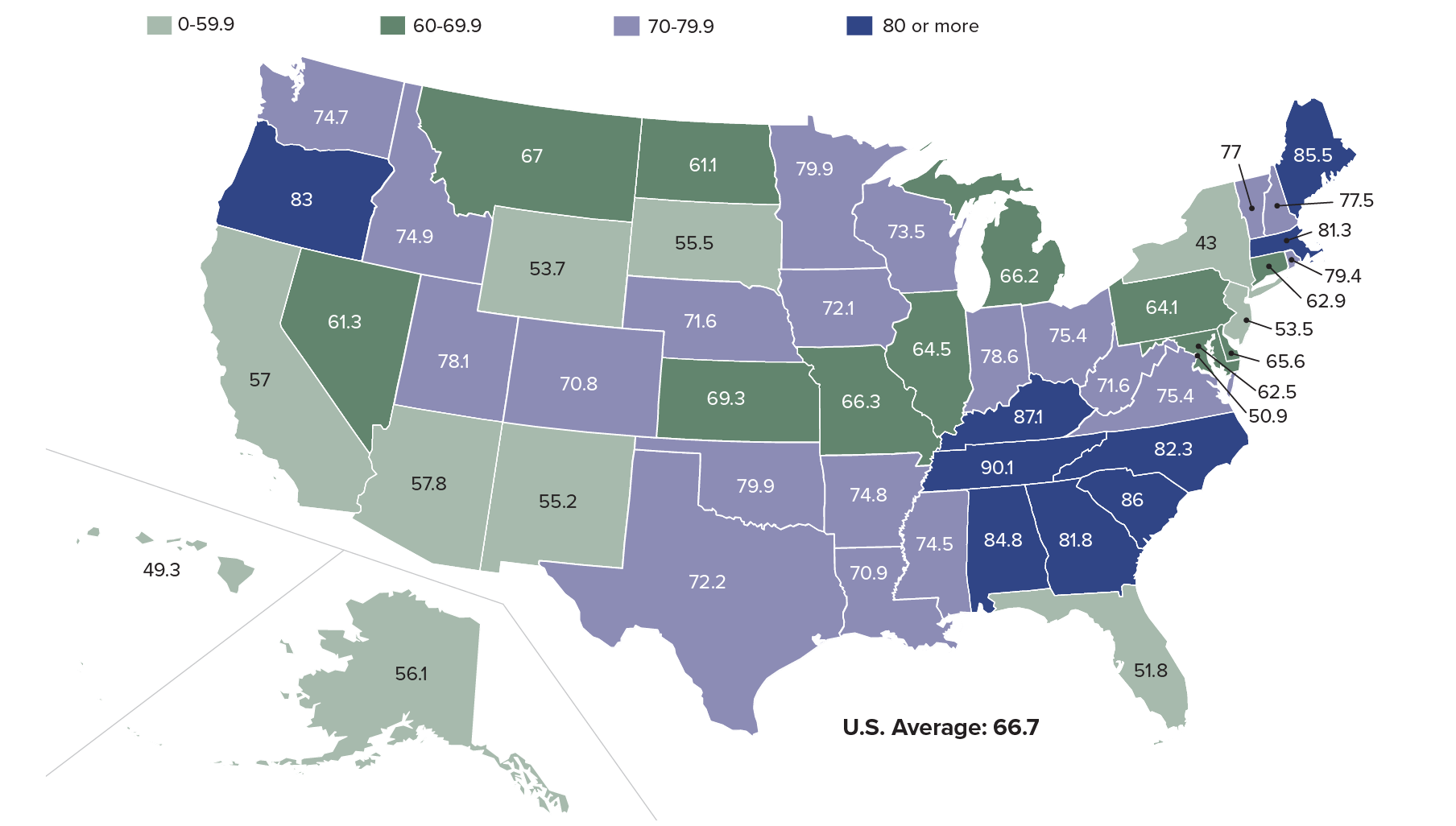
Source: Ellen A. Kramarow and Betzaida Tejada-Vera, “Dementia Mortality in the United States, 2000-2017,” National Vital Statistics Reports 68, no. 2 (2019).
Socioeconomic and Demographic Characteristics of Medicare Enrollees Ages 65 and Older With Advancing Dementia, by Care Setting
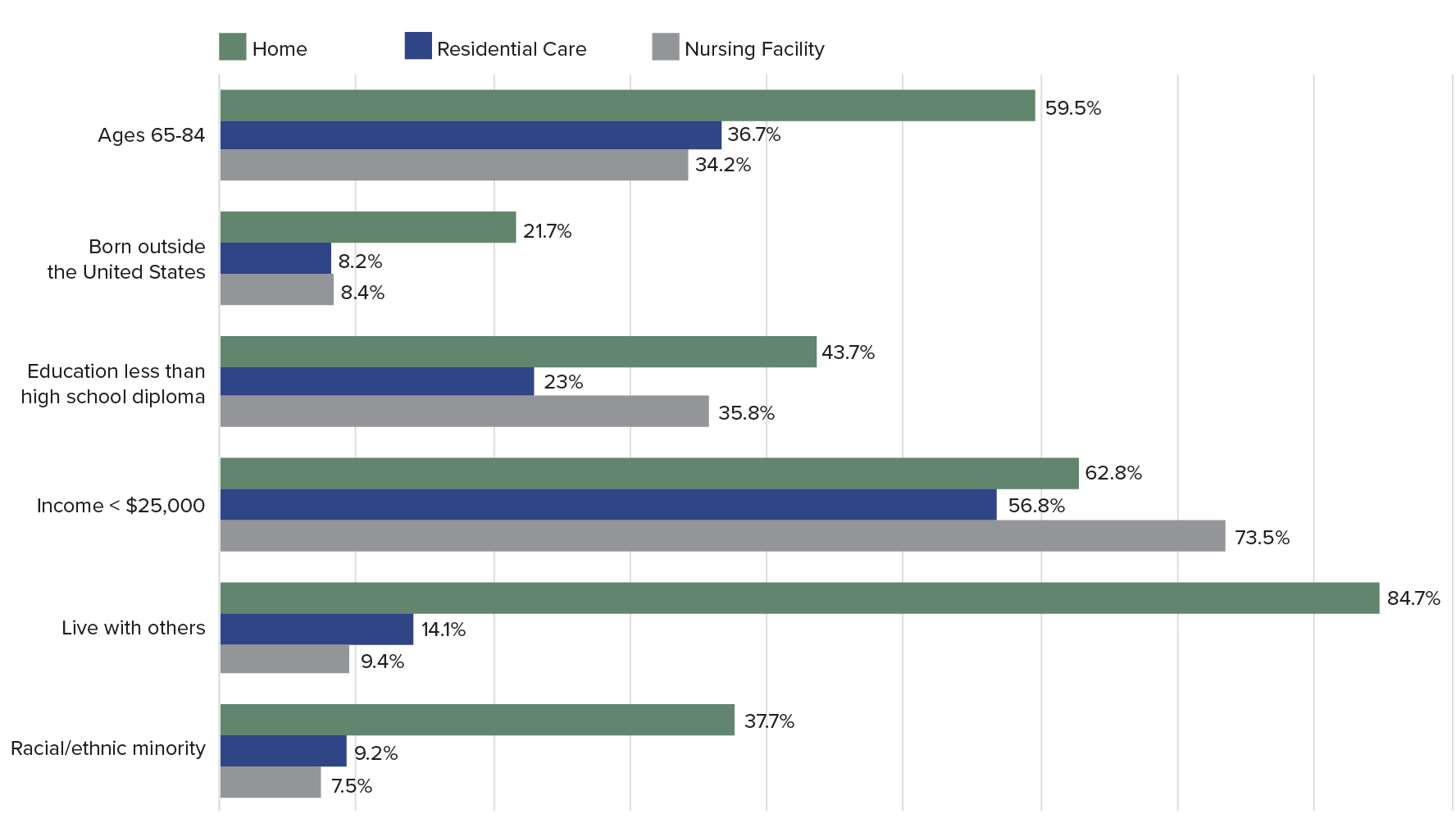
Notes: All differences comparing home versus residential care versus nursing home significant at P > .05. The amount used in many states in 2012 to determine eligibility criteria for Medicaid-paid nursing home care was $25,000.
Source: Krista L. Harrison et al., “Care Settings and Clinical Characteristics of Older Adults With Moderately Severe Dementia,” Journal of the American Geriatric Society 67, no. 9 (2019): 1907-12.
Out-of-Pocket Expenditures on Dementia During the Last Five Years of Life as a Percentage of Wealth, by Population Subgroup
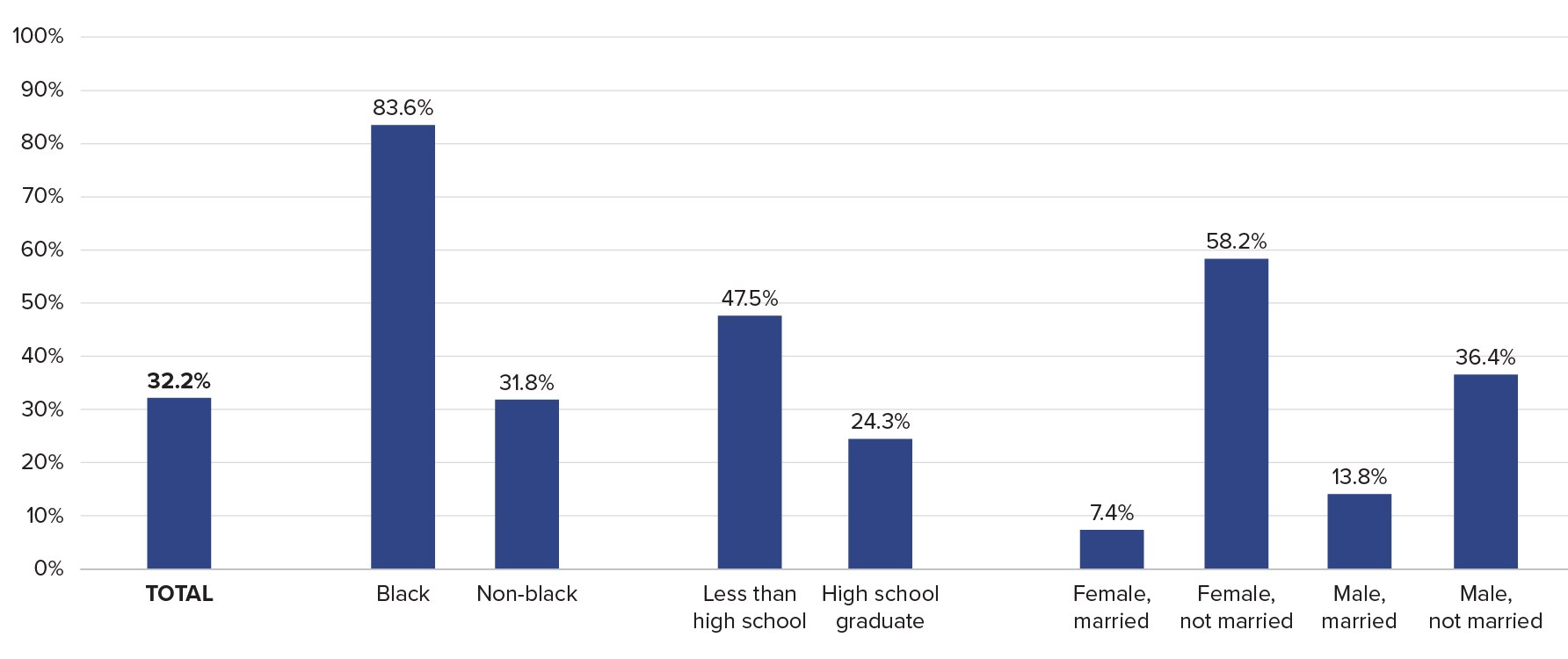
Source: Amy Kelley et al., “The Burden of Health Care Costs for Patients With Dementia in the Last Five Years of Life,” Annals of Internal Medicine 165, no. 3 (2015): 729-36.
 ">
">


