Three New Frontiers of the Mortality Paradigm
What’s killing many of us—and how we're addressing it—is changing.

Are you lucky enough to belong to a WhatsApp chat with messages like these? What started as eyeroll-inducing chatter from my extended family grew into an inside joke with my cousins and, ultimately, a lesson on mortality and connection.

Two recent messages from the author’s family WhatsApp group. The first translates to “Stay healthy, stay cool. May your day be filled with happiness.” The second reads: “Life is a poem, keep humming to its tune. There will be a thousand obstacles, but keep smiling through them all.”
Increasingly, our understanding of mortality is shaped not just by the absence of disease but also the presence of social connection. Daily calls with my parents in India inevitably include health updates about a family member, friend, or acquaintance. What I once dismissed as digital clutter is instead a form of informal health infrastructure—one that reflects a broader shift in what determines who lives, how long, and how well.
The defining global mortality story of the decade has been COVID-19—which killed an estimated 18.2 million people from January 2020 to December 2021—but the broader trajectory of human survival tells a more hopeful story. Decades of progress in medicine, sanitation, and living standards have driven rising life expectancy and widespread population aging, among the greatest public health achievements of our time. After pandemic-related setbacks, global life expectancy rebounded to over 73 years in 2024.
While challenges like infant and maternal mortality and infectious diseases persist, and climate change acts as a threat multiplier by intensifying environmental hazards that destabilize communities and exacerbate the lethal impacts of air pollution, what’s killing many of us is changing. In the 20th century, mortality was shaped largely by infectious disease. In the 21st, it is increasingly molded by three emerging frontiers: social connection, metabolic health, and biological aging. The challenge is no longer merely surviving—but aging well in a world where longevity is the norm.
The First Frontier: Socializing as Medicine
Today’s thinking on mortality recognizes that social connection is not a luxury: it is a determinant of survival. Those Good Morning GIFs and prayer chains, it turns out, are prosocial behaviors in the truest sense. WhatsApp is enormously popular among older adults worldwide, and it has been shown to combat depression, dementia, and loneliness. The chats also serve as an informal welfare check—a sudden silence, a missing “good morning” can be a distress signal to everyone watching.
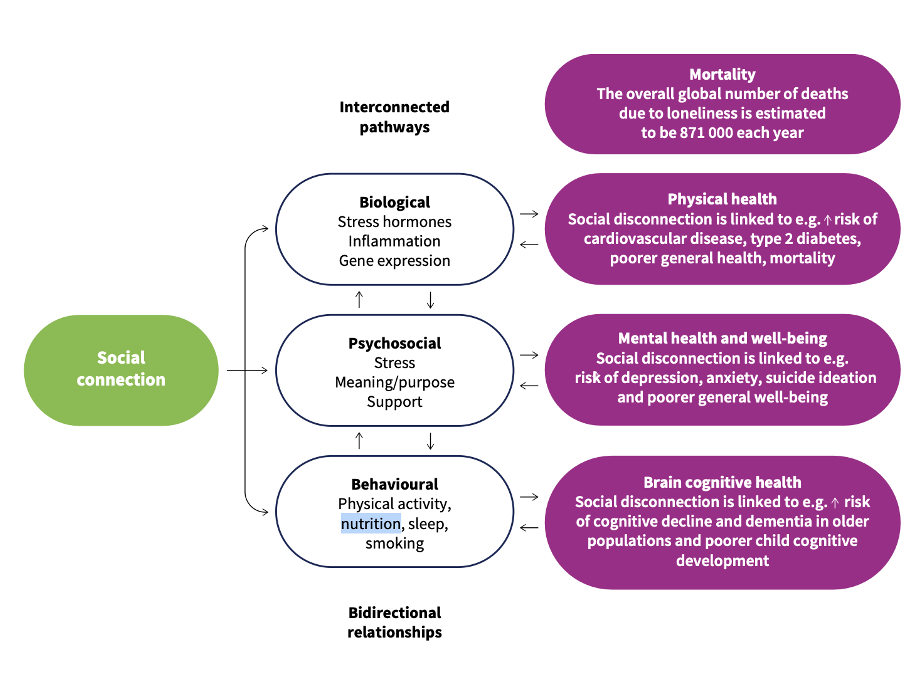
The scale of the problem is hard to ignore. In 2023, U.S. Surgeon General Dr. Vivek Murthy declared a loneliness epidemic, warning of its devastating consequences—a 29% higher risk of heart disease, a 32% increased risk of stroke, and a 50% increased risk of dementia for older adults. The WHO Commission on Social Connection has since confirmed the global scope: 1 in 6 people worldwide experience loneliness, linked to roughly 871,000 deaths annually (see Figure 1). PRB’s own analysis adds that older adults’ social ties are more important for physical and social health than previously thought.
Figure 1. Three Main Causal Pathways from Social Connection to Health
The picture is more complex for younger adults, who are more connected than ever but may also be lonelier. The research remains nascent and more nuanced than the alarmist media coverage suggests. While some studies link addictive screen use to worse mental health and suicidal ideation, others find social media a vital place for young people—one that fosters the active communication essential for healthy development.
The crisis cuts deepest in the Global South, where 24% of people report loneliness—double the rate of high-income nations. This shatters the myth that loneliness is a disease of affluence, revealing instead how economic instability, migration, and displacement fray the social fabric. Here, prosocial buffers become critical. The 2025 World Happiness Report suggests that a 10% increase in community prosociality—WhatsApping, donating, volunteering—can measurably reduce “deaths of despair,” which disproportionately affect older people. As we move toward 2030, our ability to address social disconnection may be as fundamental to addressing mortality as any clinical intervention.
The Second Frontier: Centering Metabolic Health
The second frontier is metabolic health, where rising obesity and new pharmaceutical interventions are reshaping mortality at a global scale.
The WHO reports that 16% of adults worldwide lived with obesity in 2022—double the 1990 rate. Obesity raises the risk of cardiovascular disease, type 2 diabetes, musculoskeletal disorders, and certain cancers, and contributes to one in ten infectious disease deaths. The economic toll is equally stark. By 2060, the global impact is projected to rise from $2 trillion to $18 trillion—over two-thirds of it driven by lost productivity from premature death and disability—with low- and middle-income countries bearing the greatest burden.
The early 2020s marked a turning point. GLP-1 drugs—such as semaglutide and tirzepatide, originally developed for diabetes—are now recognized for significant weight loss benefits and measurable reductions in all-cause mortality. While still relatively new, these therapies have been shown to reduce all-cause mortality by 14-21% in certain high-risk populations. The landmark SELECT trial linked semaglutide to a 20% drop in the risk of heart attack, stroke, or cardiovascular death. Long-term population-level impacts—and equity implications—remain uncertain, but these early results are promising.
For employers, the calculus is significant. GLP-1 medications carry significant upfront costs—often exceeding $1,000 per month and driving a 50% surge in pharmacy spending—but can function as a strategic investment. By reducing obesity-related absenteeism, which costs U.S. employers $4.3 billion annually, and cutting cardiovascular hospitalizations by 37%, GLP-1s help stabilize human capital. Notably, 31% of employees would consider switching jobs for this coverage.
Still, the WHO cautioned in December 2025 that medication alone cannot solve the global obesity crisis. While GLP-1s were added to the Essential Medicines List last year, they are projected to reach fewer than 10% of those who need them. High prices are limiting access to these medicines. Expanding access will require prioritizing the highest-need patients, encouraging generic competition, and making these treatments available in primary care—especially in underserved areas.
The Third Frontier: Slowing Aging With Science
The third frontier moves deeper still—targeting aging itself as a modifiable biological process.
A growing shift in the mortality paradigm is the move from reactive treatment to proactive management. Rather than treating age-related diseases as isolated and inevitable, emerging science reframes aging as the primary driver of chronic illness—and therefore a target for intervention. Geroscience, a rapidly evolving field, focuses on the underlying biological mechanisms of aging—inflammation, epigenetic change, and metabolic dysfunction—that shape our vulnerability to disease. By intervening at this level, researchers aim to address root causes rather than downstream conditions like heart disease, cancer, or Alzheimer’s.
Figure 2. Geroscience
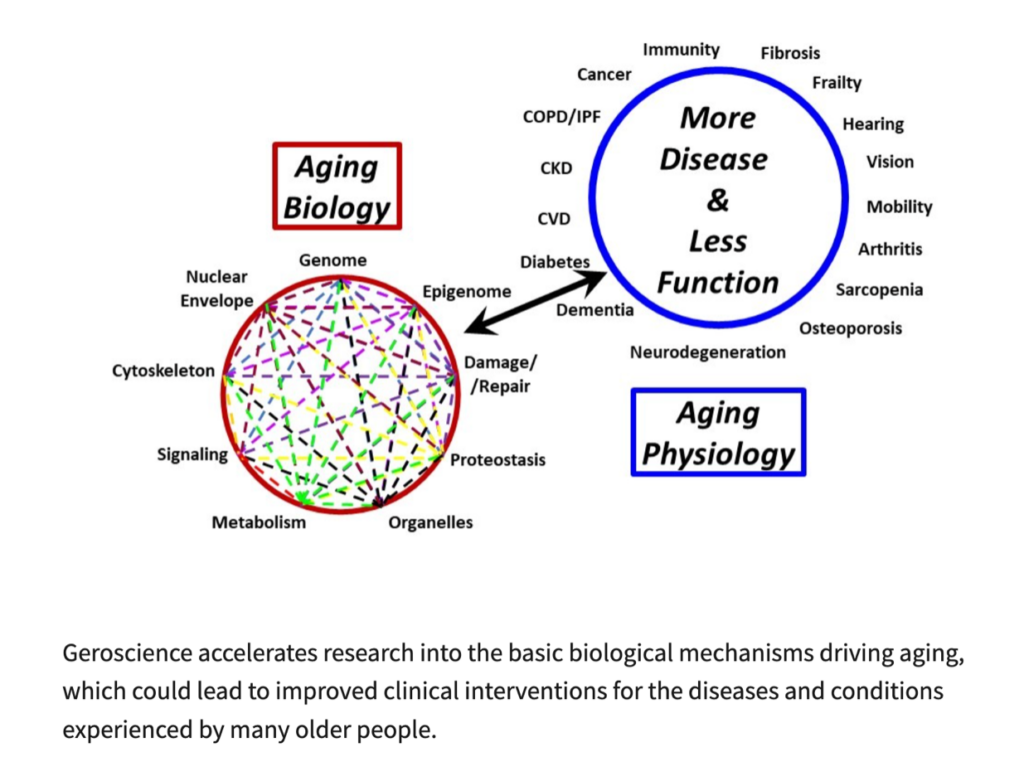
Source: National Institute on Aging.
Unlike “biohacking”—the Silicon Valley-popularized approach of DIY health optimization—geroscience is rooted in peer-reviewed clinical research and systems biology. Longevity medicine is increasingly using high-resolution diagnostics, like epigenetic clocks and continuous metabolic monitoring, to move beyond generic population-level health guidelines and toward personalized interventions. The goal is to treat our biology as an operating system that can be optimized for resilience, rather than a static fate to be endured.
The risk, of course, is access. If geroscience’s tools remain exclusive, they will deepen existing inequities in diagnosis, treatment, and outcomes. The true measure of its success will be whether these breakthroughs become a universal standard of human health—or a high-tech luxury that widens the divide in global mortality.
Looking Toward the Future
The future of mortality will not be determined by medicine alone, but by whether we can build societies that are connected, equitable, and resilient—both biologically and socially. So the next time your phone lights up with a “Good Morning” message, consider it not as noise, but as a small act of survival.
Related Posts
Pandemic Prompts New Digital Health Solutions for Family Planning
How programs in India, Nigeria, and Uganda embraced new technology to deliver family planning and maternal health services emphasizing self-care throughout COVID-19.
Adolescents and Youth Are Key to Fully Achieving Universal Health Coverage
In 2021, adolescents and youth between ages 10 and 24 are estimated to make up approximately 24% of the world’s population.

Aging and Health in China: What Can We Learn From the World’s Largest Population of Older People?
The United Nations projects that there will be 366 million older Chinese adults by 2050, which is substantially larger than the current total U.S. population of 331 million.
