Medicaid Cuts Could Push Vulnerable Older Adults Into Nursing Homes

Medicaid cuts enacted under the One Big Beautiful Bill Act (H.R. 1, Pub. L. 119-21)—many of which are being phased in over time—could affect about 1 million older adults enrolled in both Medicare and Medicaid who need help with basic activities such as bathing, dressing, and eating.
These dual-eligible older adults are old enough to qualify for Medicare but have incomes and assets low enough to also qualify for Medicaid. Medicare pays for medical care but provides minimal long-term care benefits. Medicaid helps fill this gap, covering the daily assistance many older adults need to remain safely in their homes.
Research funded by the National Institute on Aging highlights what is at stake. Together, the findings suggest that reducing Medicaid-funded home care could shift care responsibilities onto families and increase nursing home entry, increasing costs and intensifying strain on family caregivers.
The dual-eligible population lives on the edge
Remaining in the community as one gets older—a concept commonly called “aging in place”—typically depends on extensive support. Andrew Jopson and colleagues at Johns Hopkins University examined older adults enrolled in both Medicare and Medicaid who need help with two or more daily living activities (dressing, bathing, or using the toilet).1 They found that nearly 80% of these individuals receive help from two or more caregivers and receive more than 70 hours of care per week from both paid workers (often funded by Medicaid) and family members. Despite their high needs, 75% live in the community: 58% with family or others and 16% alone. The remaining 25% reside in residential care facilities or nursing homes.
These dual-enrolled individuals face compounding vulnerabilities: Nearly 70% report fair or poor health, 40% have probable dementia. Further, they average 3.6 chronic conditions, such as diabetes, cardiac issues, and cancer. Even with dual coverage from both programs, most have very limited financial resources to cover their care needs.
Where you live shapes the care you receive
Geographic location plays a major role in dual-eligible older adults’ access to coordinated care, the Jopson study found. More than half (56%) live in areas where states contract with managed care organizations to deliver managed long-term services and supports (MLTSS) programs, which provide care coordinators to help navigate services and connect medical care with daily assistance. The remaining 44% receive services through traditional fee-for-service Medicaid, which generally offers no care coordination, leaving individuals and families to arrange disparate services on their own.
MLTSS access follows stark racial and geographic patterns (Figure 1). Hispanic dual-eligible older adults are much more likely to live in areas with coordinated care. They make up 50.5% of dual-eligible individuals in MLTSS areas, compared with 15.1% in areas without these programs. Black dual-eligible older adults face the reverse: they represent just 11.6% of those in MLTSS areas but 25.4% in areas where no coordinated care programs exist.
Rural dual-eligible older adults have the least access to coordinated care. Only 8.7% of dual-eligible individuals in MLTSS areas live in rural locations compared to 31.4% in non-MLTSS areas. Rural communities also have 35% fewer home health aides per older resident than urban areas.
Fewer dual-eligible older adults live in nursing homes in MLTSS areas (18.4%) than in areas without MLTSS (34.7%)—though whether MLTSS programs enable community living or these areas simply have different regional characteristics remains unclear.
Figure 1. Among High-Need Older Adults, Hispanic Individuals Are More Likely To Live in Areas With Coordinated Care
Demographics of dual-eligible older adults with high care needs living in areas with and without MLTSS programs
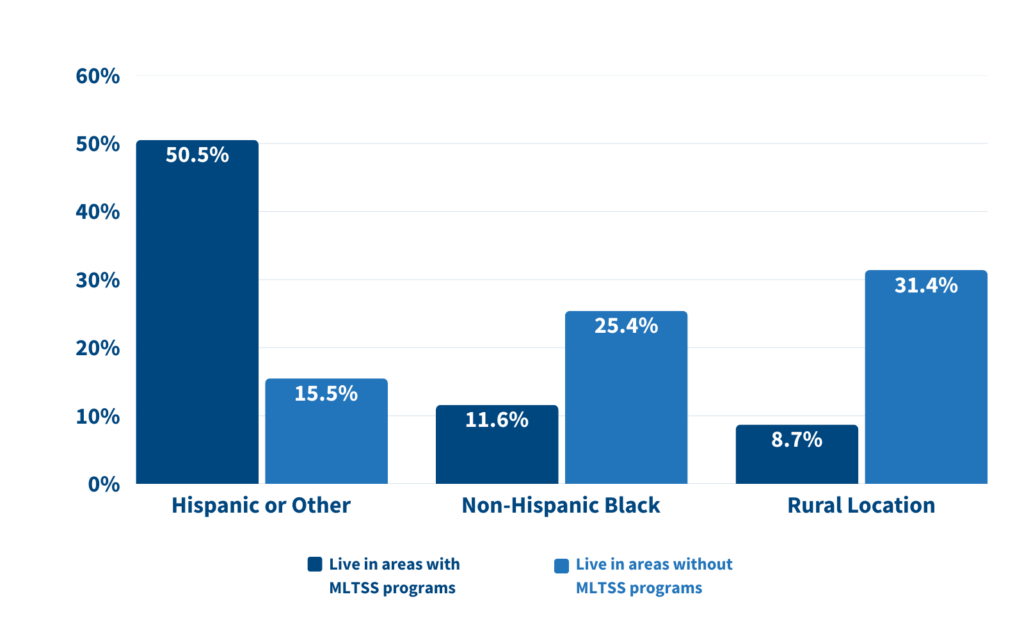
Source: Andrew D. Jopson et al., “Profile of Older Dual-Enrollees Living in Areas with Managed Long-Term Services and Supports,” Journal of the American Medical Directors Association 25, no. 4 (2024): 722–8.
Beyond program structure, local resources shape care access. Research by Chanee Fabius and colleagues at Johns Hopkins University found that service availability, workforce capacity, transportation, housing affordability, and state policies determine whether older adults with disabilities get the help they need.2
When care needs go unmet, the consequences can be serious. Older adults with disabilities may be unable to bathe, dress, eat, or move around safely. They may miss medications, remain in soiled clothing, or be unable to leave their homes. These unmet needs can increase the risk of falls, emergency room visits, hospital stays, and declining health.
Those in higher-poverty neighborhoods are more likely to experience adverse consequences when their care needs aren’t met. In these neighborhoods, 42.9% of older adults report negative consequences, compared with 34.1% in low-poverty areas.
State investment in home care also matters. In states with the lowest home care spending, 45.5% of older adults with disabilities who receive assistance report being unable to visit friends and family, attend religious services, or participate in club meetings and activities they consider important, compared with 36.1% in states with higher spending.
Strict financial rules already limit access to care
Dual-eligible older adults qualify for Medicaid coverage of medical care, but qualifying for Medicaid payment of long-term services and supports requires passing additional, stricter tests for income, assets, and home equity. Research by Robert Hest and colleagues at the University of Minnesota shows how restrictive these rules already are.3 Only about one in five older adults—about 10 million people—meet all financial criteria (Figure 2). Most states limit countable assets to just $2,000 for individuals, forcing people to exhaust nearly all savings before receiving help.
Figure 2. Just 1 in 5 Adults Meet All Requirements for Medicaid Long-Term Services and Support
Share (and number, in millions) of U.S. adults ages 65+ who meet criteria for MLTSS
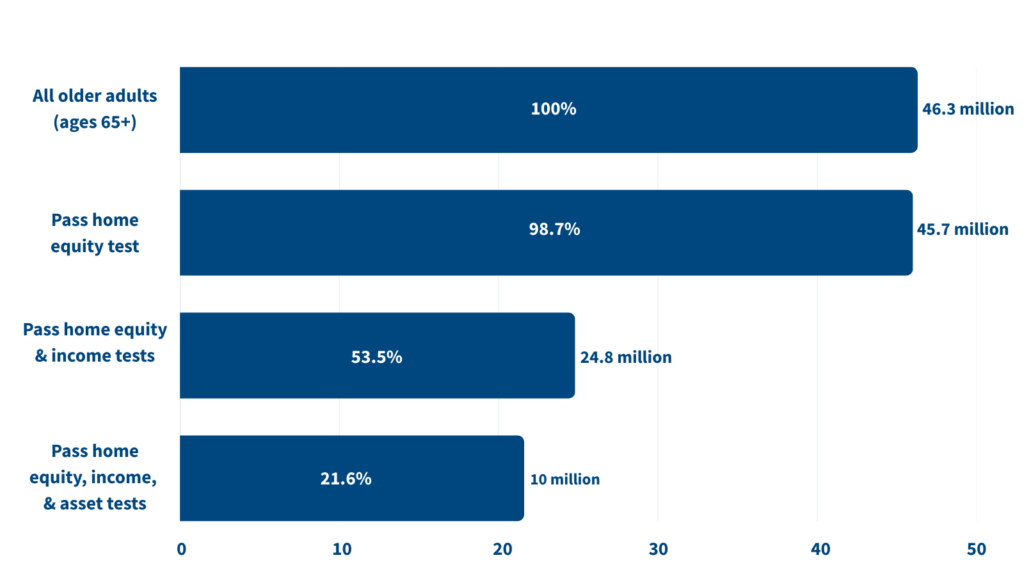
Source: Robert Hest et al., “Modeling Financial Eligibility for Medicaid Long-Term Services and Supports,” Journal of Aging & Social Policy 34, no. 6 (2022): 923–37.
The researchers modeled what would happen if states adopted the most restrictive rules used anywhere in the country. Under this scenario, 6.8 million older adults, including many dual-eligible individuals, would lose eligibility for long-term services and supports. These individuals have significant care needs: 17.3% have limitations in two or more daily activities, 48.3% report fair or poor health, and 33.3% have cognitive impairment. Even small differences in income or savings determine whether someone qualifies, and further tightening eligibility rules would exclude millions of older adults with substantial disabilities and health problems who need long-term care services.
These findings suggest that even small changes in eligibility criteria could have significant consequences for older adults with high care needs.
Why nursing home care is easier to access than help at home
The Hest study shows that Medicaid often makes expensive nursing home care easier to access than more affordable home care.
This imbalance reflects federal rules that require states to cover nursing home care but make coverage of home- and community-based services optional. As a result, states frequently apply stricter financial requirements to home care than to institutional care.
The cost difference is substantial. Home care costs approximately $46,000 per year on average—nearly half the $82,000 to $92,000 annual cost of nursing home care4. Yet state policy choices can make the cheaper option harder to access. When facing budget pressures, states have often cut home services through enrollment caps, waiting lists, or reduced hours while continuing to fund mandatory nursing home coverage. The result: Medicaid’s structure pushes people toward institutional care that costs substantially more than supporting them at home.
Figure 3. Nursing Home Care Costs Nearly Twice as Much as Home Care for Dual-Eligible Older Adults
Average annual cost of long-term care for U.S. adults ages 65+ who are eligible for both Medicaid and Medicare
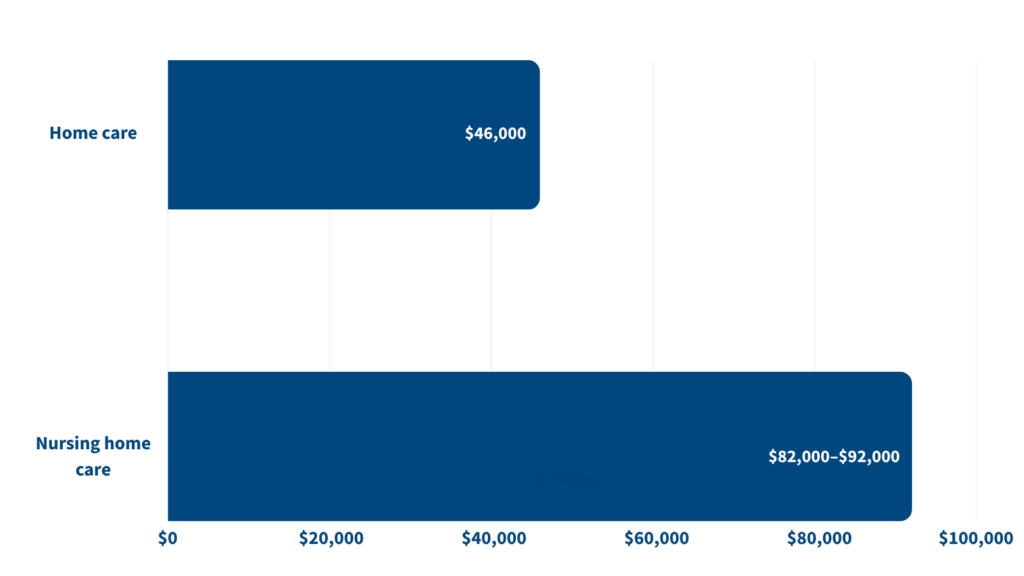
Source: Kirsten J. Colello, “Medicaid Financial Eligibility for LTSS (Report No. R43506),” Congressional Research Service, March 7, 2017, as reported in Hest et al., “Modeling Financial Eligibility for Medicaid Long-Term Services and Supports,” Journal of Aging & Social Policy 34, no. 6 (2022): 923–37.
Caregiving capacity is already under strain
Family caregivers already provide most long-term care in the United States. Among all older care recipients, 69% receive only informal care from family or friends, while just 5% rely solely on paid help.
This heavy reliance on family caregivers occurs as the pool shrinks dramatically: By 2040, the Census Bureau projects there will be just three potential family caregivers per person age 80 or older, down from six in 2025—a 50% decline in 15 years. Meanwhile, the number of adults ages 85 and older will triple by 2050, creating an unprecedented mismatch between care needs and caregiver availability.
The paid care workforce faces parallel pressures. The Fabius study found that older adults in areas with the lowest direct care worker wages (under $10.29 per hour) experienced greater restrictions on valued activities compared to those in areas with higher wages ($11.26 to $14.69 per hour). When Medicaid cuts reduce paid services, dual-eligible older adults and their families must absorb more care responsibilities even as both caregiver availability and paid workforce capacity simultaneously decline.
Looking ahead
The three studies reveal the risk ahead as Medicaid cuts under the One Big Beautiful Bill Act take effect. Dual-eligible older adults already face substantial barriers: strict financial eligibility rules, geographic disparities in service access, and dependence on a shrinking pool of family caregivers and paid workers. If states respond to reduced federal funding by tightening eligibility, the cuts will disproportionately affect those with the highest care needs—older adults with greater functional limitations, poorer health, and higher rates of cognitive impairment.
The outcome is predictable: Cutting home care services could push more dual-eligible older adults into nursing homes that cost Medicaid substantially more, increasing rather than decreasing state spending. These cuts will hit hardest those with the greatest needs—particularly older adults living in rural areas and high-poverty neighborhoods with fewer services—and will accelerate institutionalization precisely when families and the care system are already under strain. Few states have significantly tightened long-term care eligibility in recent years, instead seeking ways to support independent living. The research shows that further restrictions on home care would harm the very people the program exists to serve.
Taken together, the findings highlight practical policy approaches that can better support aging in place and reduce reliance on nursing homes. States that have invested in home and community-based services, supported family caregivers with paid leave, and raised wages for direct care workers have seen improved outcomes for dual-eligible older adults—while simultaneously reducing costly nursing home placements. Community-based programs such as CAPABLE (Community Aging in Place—Advancing Better Living for Elders) show that modest investments in home modifications and supportive services can help lower-income older adults remain safely and independently at home.
Rather than cutting Medicaid’s long-term care supports, the researchers recommend strengthening the program through a social insurance approach that spreads costs more equitably across generations. As Hest and colleagues caution, “the Medicaid program for LTSS among the 65+ population is already well targeted and restricting eligibility would likely exclude individuals in need of services.” The evidence suggests that protecting and expanding home-based care is not only a more equitable approach, but also a more fiscally sustainable one as the U.S. population ages.
References
- Andrew D. Jopson et al., “Profile of Older Dual-Enrollees Living in Areas with Managed Long-Term Services and Supports,” Journal of the American Medical Directors Association 25, no. 4 (2024): 722–8.
- Chanee D. Fabius et al., “The Role of Place in Person- and Family-Oriented Long-Term Services and Supports,” Milbank Quarterly 101, no. 4 (2023): 1076–138.
- Robert Hest et al., “Modeling Financial Eligibility for Medicaid Long-Term Services and Supports,” Journal of Aging & Social Policy 34, no. 6 (2022): 923–37.
- Kirsten J. Colello, “Medicaid Financial Eligibility for LTSS (Report No. R43506),” Congressional Research Service, March 7, 2017
Related Posts
As Dementia Rises, More Older Americans Are Getting Care at Home. It's Not Without Challenges.
Families face the financial burden of paying out-of-pocket for care not covered by Medicare and Medicaid and the emotional toll of day-to-day caregiving.

Webinar: How Women Became America’s Safety Net (PRB Book Talk)
A conversation with author Jessica Calarco on her new book, Holding It Together

The Demography of Dementia and Dementia Caregiving
Dementia is one of the nation’s most expensive old-age health conditions and the most time consuming for family caregivers.

Family Caregiving for Older People
(2016) In the United States, the vast majority of care that allows older people to live in their own homes is provided by family members who do not receive pay for their services.
