When Doctors Advise Teens on Contraception, Bias May Shape the Conversation

For many teenagers, a conversation with their doctor is the primary way they learn about contraceptive options. One talk can shape both the methods they choose and their confidence in seeking future care.
A new study suggests that when doctors counsel teenagers about birth control, their recommendations may be influenced by more than just medical evidence. In a survey of nearly 300 clinicians, researchers presented fictional patient scenarios, then asked providers to rank which contraceptive methods they would recommend.
Doctors most often recommended long-term birth control methods, like IUDs and implants, found a team lead by Dr. Bianca A. Allison (University of North Carolina School of Medicine). But their recommendations shifted depending on the situation and the patient.
In explaining their choices, many clinicians emphasized concerns about teenagers’ ability to consistently use short-term methods like the pill. Only 1% of responses mentioned patient choice or shared decision-making—a finding the researchers say contradicts clinicians’ ethical responsibility to guide rather than direct their patients’ choices.
How Clinicians Ranked Contraceptive Options
Across all scenarios, clinicians ranked long-acting reversible contraceptives, or LARCs, as their top recommendation in about six out of 10 cases (see figure). These methods—intrauterine devices (IUDs) and implants placed under the skin of the arm—are among the most effective forms of birth control and can prevent pregnancy for several years.
Figure 1. Clinicians Recommended Long-Acting Contraceptive Methods for Adolescents More Often Than the Pill, Ring/Patch
Percentage of survey scenarios in which clinicians ranked each contraceptive method first
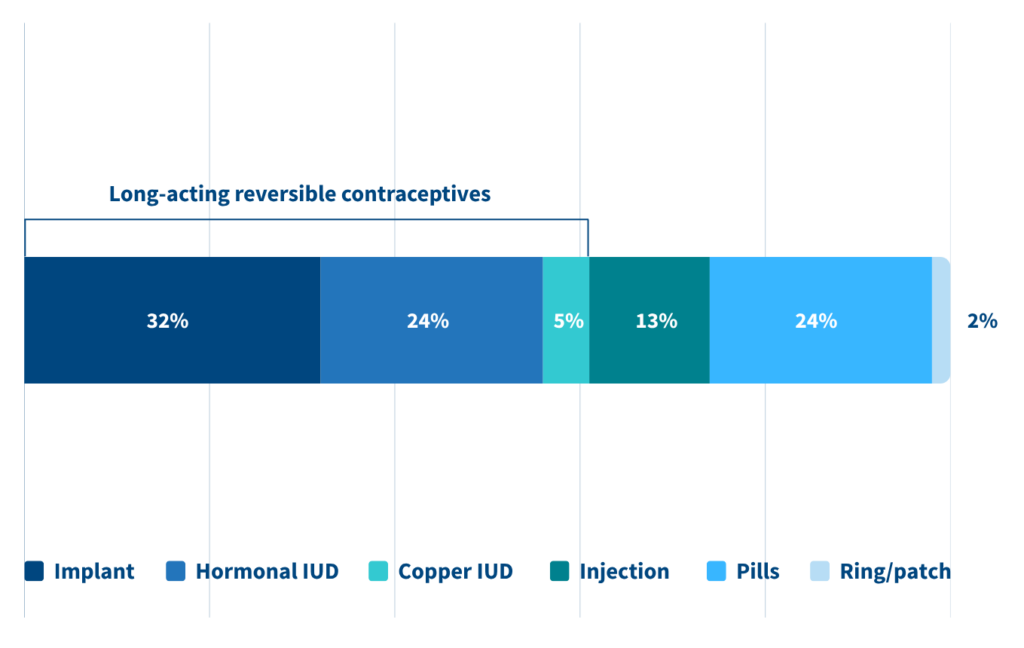
Source: Bianca A. Allison et al., “Exploring Primary Care Physician Biases in Adolescent Contraceptive Counseling,” Contraception 141 (2025): 110706.
Still, recommendations varied depending on the patient. Clinicians were less likely to recommend LARCs for a 14-year-old than a 17-year old; they were less likely to recommend them for Hispanic patients and more likely to recommend them teens who had already been pregnant.
Most of the clinicians surveyed practiced pediatrics. While many said they were familiar with current contraceptive guidelines, only 17% said they inserted IUDs themselves, pointing to differences in clinical training and experience.
Clinical recommendations for LARCs have changed with major medical organizations now saying that young age or a history of pelvic infection are no longer reasons to avoid them. Differences in how familiar clinicians are with the updated guidelines may help explain why recommendations vary, the researchers said.
Clinicians Emphasized Effectiveness, Ease of Use
The researchers also reviewed the clinicians’ written explanations for their choices. Many pointed to effectiveness and consistent use as key factors in recommending a method. Concerns about whether patients would take a pill daily were common, as were mentions of ease of use and reversibility.
About two-thirds of explanations included assumptions, such as generalizations about teens’ reliability or maturity. Far fewer (18%) focused only on clinical factors like side effects or medical eligibility. Just 1% mentioned patient choice or a patient-centered care.
Guidelines Shift Toward Patient-Centered Care
Professional guidance on contraceptive counseling has shifted in recent years. Earlier recommendations often supported “tiered-effectiveness” counseling, where providers discuss the most effective birth control methods first. More recent guidance from major medical organizations including the American Academy of Pediatrics and the American College of Obstetricians and Gynecologists now emphasizes person-centered counseling, which prioritizes a patient’s values and preferences and has been associated with higher satisfaction with both the counseling experience and the chosen method.
The continued prominence of long-acting methods in clinicians’ recommendations in this study may suggest that earlier counseling approaches remain influential in practice, even as guidelines evolve, the authors said. They note that pediatrics has been slower than other specialties to adopt person-centered approaches to contraceptive counseling.
What This Means for Care
The authors stressed that their study did not examine clinicians’ intentions. Instead, they highlight measurable patterns in recommendations and reasoning. They suggest that more attention to counseling approaches, clinician education, and awareness of potential bias may help support equitable, patient-centered contraceptive care for adolescents.
By showing how recommendations changed based on patient characteristics, the study highlights the need to look not just at which methods are offered, but how those conversations take place.
Reference
- Bianca A. Allison et al., “Exploring Primary Care Physician Biases in Adolescent Contraceptive Counseling,” Contraception 141 (2025): 110706.
Related Posts
As Dementia Rises, More Older Americans Are Getting Care at Home. It's Not Without Challenges.
Families face the financial burden of paying out-of-pocket for care not covered by Medicare and Medicaid and the emotional toll of day-to-day caregiving.

Webinar: How Women Became America’s Safety Net (PRB Book Talk)
A conversation with author Jessica Calarco on her new book, Holding It Together

The Demography of Dementia and Dementia Caregiving
Dementia is one of the nation’s most expensive old-age health conditions and the most time consuming for family caregivers.

Family Caregiving for Older People
(2016) In the United States, the vast majority of care that allows older people to live in their own homes is provided by family members who do not receive pay for their services.
