Is Medicare Advantage Really an Advantage?

More than half of people with Medicare are now enrolled in Medicare Advantage, up from about one in five two decades ago. A private-plan alternative to traditional Medicare, the newer program is increasingly important to older adults’ ability to find and afford care and services.
Proponents of Medicare Advantage cite lower premiums, built-in prescription drug benefits, and coverage for services not included in government-run Medicare insurance, like dental, vision, and hearing—benefits that are especially important for people with complex health conditions like dementia. Today, more than 34.1 million Americans are beneficiaries.
But does Medicare Advantage deliver better care than traditional Medicare? Three recent studies funded by the National Institute on Aging revealed differences in care for Medicare Advantage beneficiaries, including a higher rate of dementia diagnoses, longer hospital stays, and more at-home care at the end of life. These findings highlight the importance of understanding the relationship between payment and management rules and the care older adults ultimately receive.
Dementia diagnoses increased after payment rules changed
After a 2020 rule change boosted payments to Medicare Advantage plans for dementia patients, dementia diagnoses rose faster among Medicare Advantage enrollees than traditional Medicare enrollees, Sidra Haye (University of Southern California) and colleagues report.
The rate of new dementia diagnoses rose 11.5% in Medicare Advantage relative to traditional Medicare when the Centers for Medicare and Medicaid Services reintroduced Alzheimer’s disease and related dementias to the Medicare Advantage risk-adjustment payment model. Data are based on Medicare records for all beneficiaries in both programs from 2016 to 2020.
The increase in diagnoses after the policy change may reflect better dementia detection. It may also represent overdiagnosis or upcoding. While the paper cannot completely separate the two, the researchers find that the uptick in diagnoses was concentrated among groups that have historically been underdiagnosed, including Black and Hispanic beneficiaries, people with lower incomes, and adults ages 85 and older.
“These findings suggest that the policy change, at least in part, improved dementia detection and had the intended impact of compensating plans for the higher health care needs and expenditures of beneficiaries with dementia,” said Haye.
More evidence is needed to determine whether the increase in diagnoses has improved care or mainly increased Medicare spending.
Hospital stays grew longer for Medicare Advantage patients
After the pandemic, the length of hospital stays grew more for patients with Medicare Advantage plans than traditional plans, especially among those needing skilled nursing care after discharge, according to another recent study.
From 2017 to 2023, average time in the hospital increased by more than one day (from 6.0 to 7.1 days) for Medicare Advantage patients, while growing by half a day (from 5.8 to 6.3 days) for patients with traditional Medicare. While stays got longer for both groups, increases were significantly longer among Medicare Advantage patients, especially for extended stays of 14 days or more.
“Collectively, our results suggest that patterns of care in Medicare Advantage contributed to delays of millions of hospital days in the U.S. after 2020, with more likely in the future,” said lead author Brian McGarry (University of Rochester).
Extended stays were most common among patients discharged to skilled nursing facilities. Although the reasons for the delays are not completely understood, limited skilled nursing facility beds and administrative delays linked to prior authorization requirements are likely key factors.
From a health system perspective, extended stays are inefficient, tying up hospital beds and shifting costs to providers rather than health plans. In 2022, Medicare Advantage plans were associated with an estimated 1.9 million more hospital days than would have been expected under traditional Medicare (figure). Assuming a cost of about $3,000 per day, this additional hospital time cost health systems an estimated $5.7 billion in 2022.
Medicare Advantage Plans Are Linked to Longer Hospital Stays
Total extra days patients with Medicare Advantage spent in the hospital, compared to those with traditional Medicare, 2018–2023 (in thousands)
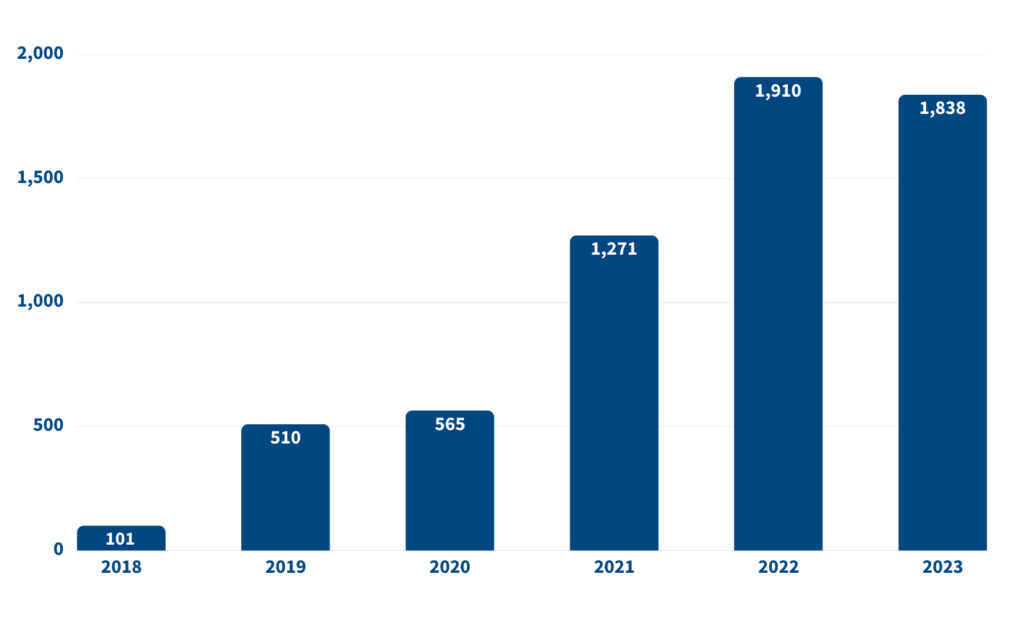
Note: 2023 estimate includes extrapolated data for October-December. Source: Brian E. McGarry et al., “Extended Hospital Stays in Medicare Advantage and Traditional Medicare,” JAMA Internal Medicine 185, no. 11 (2025): 1362–9.
But the consequences go beyond cost. Prolonged hospital stays can delay patients’ rehabilitation and recovery and increase the risk of infection, falls, delirium, and other potential harms associated with being hospitalized longer than necessary.
“These delays could have meaningful clinical implications because patients who require post-acute care are, by definition, not safe to be discharged home,” McGarry said.
End-of-life care differs between Medicare Advantage and traditional Medicare
Health plan choices shape not only how care is delivered, but also how and where people spend their final months of life.
A recent study found that Medicare Advantage enrollees received fewer Medicare-covered services near the end of life, including fewer hospitalizations and skilled nursing facility stays, than beneficiaries in traditional Medicare. Often, they received end-of-life care at home from family members or hospice.
This could mean Medicare Advantage plans are reducing unnecessary and burdensome treatments for patients receiving end-of-life care, noted lead researcher Lauren Hersch Nicholas (now at University of Colorado School of Medicine, formerly at Johns Hopkins University). Many people prefer to receive care and die at home but often end up in hospitals or nursing homes instead.
But higher rates of home-based care among Medicare Advantage beneficiaries “potentially places a large burden on family caregivers or leaves patients in need of additional services,” said Nicholas.
The findings suggest that cost-control incentives in Medicare Advantage may reduce the use of intensive, facility-based care toward the end of life, but may also leave some patients without the skilled care that they need.
Medicare enrollment is a couples’ decision
Choosing a Medicare plan is often a shared decision made within households, rather than an individual choice based solely on health needs.
Using national Medicare data, Lianlian Lei (University of Michigan) and colleagues examined how spouses and partners influence Medicare Advantage enrollment decisions.
They found that beneficiaries were substantially more likely to enroll in Medicare Advantage if their spouse or partner was already enrolled in the program. This pattern held even after accounting for health status and demographic factors, suggesting that convenience, shared providers, and coordinated coverage play an important role in plan selection.
“Policy initiatives to help beneficiaries optimize plan choice should consider that dyads frequently make enrollment choices together,” the authors conclude.
Better alignment of incentives and care is needed as Medicare Advantage grows
The researchers suggest several steps to address care gaps among Medicare beneficiaries:
- Strengthen standards so that higher payments reflect improvements in care and outcomes, not just additional diagnoses or more intensive coding.
- Improve oversight of care transitions across Medicare programs to ensure safe and appropriate discharges for all patients.
- Increase transparency about how Medicare Advantage plans manage care so beneficiaries, caregivers, and regulators can make more informed choices.
- Improve enrollment counseling so shared plan choices accurately reflect care needs, especially for couples.
Better data and evaluation tools are also needed, the researchers added. Current data limitations make it difficult to distinguish efficient care from underuse of services, report Nicholas and colleagues. Some differences between Medicare Advantage and traditional Medicare may be driven by differences in who enrolls in each program, how diagnoses are coded, or patient preferences, rather than by actual differences in care quality. Incomplete data and limited information about patients’ needs and care goals make it difficult to compare the two programs.
As Medicare Advantage becomes more common, policymakers will need stronger oversight and better information to ensure the program truly supports high-quality, fair, and patient-centered care.
References
- Sidra Haye et al., “After Risk-Adjustment Change, Dementia Diagnoses Increased In Medicare Advantage Relative To Traditional Medicare,” Health Affairs 44, no. 1 (2025): 81–9.
- Brian E. McGarry et al., “Extended Hospital Stays in Medicare Advantage and Traditional Medicare,” JAMA Internal Medicine 185, no. 11 (2025): 1362–9.
- Lauren Hersch Nicholas et al. “Medicare-Covered Services Near the End of Life in Medicare Advantage vs Traditional Medicare,” JAMA Health Forum 5, no. 7 (2024): e241777.
- Lianlian Lei et al., “Partner Plan Choices and Medicare Advantage Enrollment Decisions Among Older Adults,” JAMA 331, no. 15 (2024): 1322–5.
- Lauren Hersch Nicholas et al., “Is There an Advantage? Considerations for Researchers Studying the Effects of the Type of Medicare Coverage,” Health Services Research 59, vol. 1 (2024): e14264.
Related Posts
PRB x TED: How Do We Respond to an Aging World?
As headlines announce fewer babies and more older people the data are clear: The world is undergoing a massive demographic shift. But is demography our destiny?

Research Identifies New Strategies to Reduce Undercount of Young Children in U.S. 2020 Census
PRB identifies factors predicting where children under age 5 are more likely to be missed in the 2020 Census and develops a new undercount risk measure for young children.
