Toshiko Kaneda
Technical Director, Demographic Research

(April 2003) Reaching age 100 has long fascinated society. The century mark holds an almost mystical importance as a seal of hardiness and good health — the sign of a life well-lived. People who reach 100 are regularly feted in newspaper stories, television broadcasts, and family parties. Some get birthday greetings from the White House. As life expectancy increases, an increasing number of Americans are attaining this milestone.
Centenarians have a unique perspective on our recent history. Americans who reached age 100 in 2000 were born at the dawn of the 20th century. They were too young to participate in World War I and reached adulthood as the world was gripped by the 1918 influenza epidemic. This group was forming its families as the Great Depression started and had some of the highest rates of childlessness recorded in the United States. The advent of World War II found many of them too old to be called into service, but they were a vital force in stateside war efforts. Today’s centenarians reached retirement age as the United States entered the Vietnam War and social turmoil of the 1960s and 1970s. They witnessed remarkable and unprecedented technological and medical advances in their lifetimes.
Centenarians may hold the key to the limits of life and are a new and fascinating focus for medical and social research. Researchers are examining their physical and mental health, their genes, their families, and their lifestyles, trying to unlock the secrets of long life.
The growth in the number of centenarians in the world is remarkable. Accurate records are difficult to come by before the 20th century, although there have been claims of super longevity throughout history, such as the story of 969-year-old Methuselah in the Bible. Other examples of supercentenarian status are found in age claims of 122 years for St. Patrick of Ireland, 152 years for Englishman Thomas Parr (1483-1635), and groups of individuals in Bulgaria, Kashmir, and the Andes. Rigorous investigation of these claims, however, finds no evidence to support them. Some speculate that before 1900 the incidence of centenarians may have been as small as one per century. In small countries, like Denmark, researchers find little evidence of centenarians before the 19th century.1 Given the rarity of living to age 100, it is possible that few populations were large enough until recently to produce any centenarians.
Verification of age is very difficult, even today. Many centenarians do not have birth records or other documents to confirm their stated age. Verification of age entails collecting credible and corroborating evidence from a variety of sources, including interviews with the person when possible. Reported life events are checked for consistency with historical records and documents. Verification becomes more difficult the older the individual and after his or her death.
The oldest known age ever attained was by Jeanne Calment, a Frenchwoman who died in 1997 at the age of 122. Ms. Calment is also the only documented case of a person living past 120, which many scientists had pegged as the upper limit of the human lifespan. In April 2003, the oldest living woman appears to be 115-year-old Kamato Hongo of Japan, born in 1887. The oldest living American woman is Californian Mary Christian, age 113.
| World | United States | |
|---|---|---|
| Oldest Man | Yukichi Chuganji (Japan) | Fred Harold Hale |
| Birth date | March 23, 1889 | Dec. 1, 1890 |
| Age on April 1, 2003 | 114 | 112 |
| Oldest Woman | Kamato Hongo (Japan) | Mary Christian |
| Birth date | Sept. 16, 1887 | June 12, 1889 |
| Age on April 1, 2003 | 115 | 113 |
Source: Gerontology Research Group (www.grg.org, accessed April 2, 2003); and Guinness World Records (www.guinnessworldrecords.com, accessed April 2, 2003).
The oldest documented age for a man is believed to be a Danish immigrant to the United States, Christian Mortensen, who died in 1998 at age 115. One man, Shigechiyo Izumi, is often reported as having reached the age of 120 before his death in 1986 in Japan, but his age has not been verified. Yukichi Chuganji, reaching age 114 in 2003, is believed to be the oldest living man. Maine resident Fred Harold Hall is the oldest living American man — at 112 years of age.
Some 50,000 Americans were reported as centenarians in the 2000 U.S. Census (see figure). Centenarians account for less than 0.2 percent of the 35 million persons age 65 or older, and there is wide agreement that this is an overestimate because of chronic overreporting at the oldest ages.2 Reliable counts for 1990 by the Social Security Administration, for example, put the number of centenarians as closer to 28,000 than the 37,000 reported in the 1990 Census.
Note: Components do not add to total because of rounding.
Source: U.S. Census Bureau, PCT3 Sex by Age (http://factfinder.census.gov/, accessed April 2, 2003).
As at all other older ages, women centenarians outnumber men. The 2000 Census recorded four women for every man age 100 or older. Detailed information on centenarians from the 1990 Census reveal that their racial composition is similar to that for all older Americans — 78 percent of centenarians were non-Hispanic white and 16 percent were black. But centenarians have lower levels of education than other elderly Americans, which is not surprising for Americans born before 1900. And women age 100 or older are more likely than men to be widowed. Only about 4 percent of female centenarians counted in 1990 were currently married, compared with nearly 25 percent of the men age 100 or older.
Centenarians are not necessarily in poor health or suffering from chronic disabilities. About 20 percent of the centenarians in the 1990 Census reported no disabilities, although they reported considerably more health problems than people in their 80s.3
What accounts for extreme longevity? It is likely that a combination of genetics, lifestyle, and luck4 are responsible for a long life. As public health measures advanced early in the 20th century, cleaner water, vaccination campaigns, and better personal hygiene allowed more people to live to older ages. More recently, treatments for heart disease, cancer, and other chronic diseases have extended life at the upper extremes. A wide-ranging study of the genetic, physical, mental, and emotional characteristics of centenarians by Harvard University’s Thomas Perls suggests that genetic factors play a large role in longevity, although Perls also acknowledges the importance of lifestyle and attitude.5
Christine L. Himes is associate professor of sociology and senior research analyst at the Center for Policy Research at Syracuse University.
Excerpted from PRB’s Population Bulletin “Elderly Americans,” by Christine L. Himes.
(December 2002) Life expectancy is a hypothetical measure. It represents the average number of additional years that a person could expect to live if current mortality trends were to continue for the rest of that person’s life. But death rates do not remain fixed over time. They have fallen steadily over the past century. Between 1900 and 2000, life expectancy in the United States increased from 51 to 80 for females and from 48 to 74 for males.
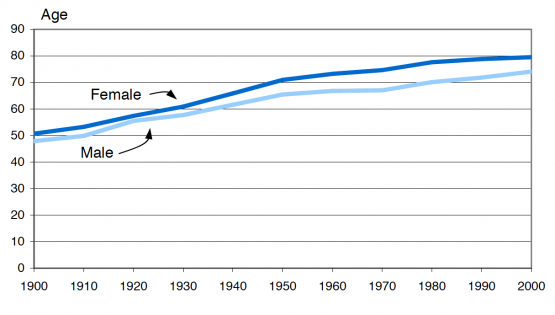
Source: AmeriStat, analysis of data from the National Center for Health Statistics.
Most of the improvements in life expectancy have resulted from reductions in infectious diseases among infants and children. The decline in mortality rates for these major killers has been attributed to improvements in public health efforts, medical technologies, and standards of living and hygiene. Today, the leading causes of death are cardiovascular disease (heart disease), malignant neoplasms (cancer), and cerebrovascular disease (stroke).
Data on long-term mortality trends have to be used with caution because, in the early decades of the 20th century, not all states participated in national death registration. Also, coverage was incomplete, especially for the poor and for racial minorities. Classification of causes of death depends on the medical knowledge and qualifications of the people attending the death. Historians have argued, for example, that many of the deaths ascribed in the early years of this century to other causes, or to indeterminate ones, were actually hard-to-diagnose cases of cardiovascular disease. The categories change over time, but the trends shown in these data for the overall risk of death and the major groups of causes are considered valid.
References
Federal Interagency Forum on Aging-Related Statistics, Older Americans 2000: Key Indicators of Well-Being (2000): Table 12A; A.M. Minino et al., “Deaths: Final Data for 2000,” National Vital Statistics Reports 50, no. 15 (2002).
(November 2000) Three quarters of older American men live in a family setting, while only half of older American women do. In 1999, 9.8 million people ages 65 and older lived alone, 77 percent of whom were women. The percentage of older people living alone increases with age. In 1999, about 15 percent of men and 31 percent of women ages 65 to 74 lived alone, but among those 75 and older, 20 percent of men and 51 percent of women lived alone. The percentage of women ages 75 and older living alone has increased by 10 percentage points since 1970.
The percentage of older people residing in institutions has been declining in recent years. According to the National Nursing Home Survey, the percentage of people ages 85 and older residing in nursing homes declined from 22 percent in 1985 to 19 percent in 1997. Among people ages 75 to 84, the percentage in nursing homes declined from 6 percent in 1985 to 5 percent in 1997. This decline may reflect the decline in disability rates among the older population, reported by several sources, and the increase in the availability of home health services over this period. Though the percentage of older people in nursing homes declined, the absolute number of older people in nursing homes increased, from 1.3 million in 1985 to 1.5 million in 1997, because the total number of older people in the population has increased.
Most of the data, charts, and graphs on the older population are based on tabulations from the Census Bureau’s March Current Population Survey (CPS).

 ">
">