- End Child Marriage by Sani Muhammad and Mubarak Idris, Nigeria.
- Let Your Voice Be Heard by Imali Ngusale, Kenya.
The Pakistan project team is funded separately by PRB.


This PIA MIMI created video on contraceptives was inspired by the Population Reference Bureau. The initiative began as an idea for meaningful youth participation given that young people’s voices are always sedated whenever it comes to highlighting their thoughts and beliefs. In this video PIA MIMI sought to deconstruct the sedation of young people’s voices and let young people speak their mind and literally take control of your future.
Young people are often judged and misunderstood for seeking information and services relating to their sexual and reproductive health. Working with a team of young people in Kaduna state with support from the Population Reference Bureau, young people are standing up to bring their issues to the fore of government priorities in accessing family planning information and services.
Child marriage is one of the biggest problems in northern Nigeria, leading many young girls to drop out of school, and contributing to the high rates of maternal and infant deaths. Working with the Population Reference Bureau, we trained a team of young sexual and reproductive health advocates who used their smartphone to amplify voices of these girls.
Meet Zainab! A mother of two who was married out as a child bride. Like Zainab, over 6 million girls in Nigeria are forced into marriage at age 15, and live with dire consequences. Hear and Share her story. #SpeakUp. Let’s join the conversation to end child marriage.

In response to the coronavirus pandemic, PRB is supporting partners and others by providing information and resources to help communities stay safe. These videos, produced for our partner, Cadres des Religieux pour la Santé et le Développement (CRSD), encourage faith communities in the Sahel region of Africa to worship at home and to adopt other practices to stem the spread of the virus in that region.

United States Ranks 53 Out of 195 Countries on Aging-Health Problems
The United States doesn’t have the world’s oldest population, but relatively high levels of age-related disease could affect the proportion of Americans who become critically ill because of COVID-19.
Older Americans on average have a higher level of age-related health problems than their counterparts in Europe and many other countries (see table). That’s according to a recent Lancet study that shows the United States ranked 53rd out of 195 countries when it comes to how burdened its people are by old age-related disease and disability.
By comparison, Switzerland ranked 1st, South Korea ranked 3rd, Italy ranked 5th, and China ranked 75th. To compare the relative health of adults among countries, the study adjusted for the wide differences in the proportion of adults in each age group in each country. For example, Italians ages 65 and older make up 23% of the population compared with 16% in the United States, 15% in South Korea, and 12% in China.
| wdt_ID | Rank | Country |
|---|---|---|
| 1 | 1 | Switzerland |
| 2 | 2 | Singapore |
| 3 | 3 | South Korea |
| 4 | 4 | Japan |
| 5 | 5 | Italy |
| 6 | 6 | Kuwait |
| 7 | 7 | Spain |
| 8 | 8 | France |
| 9 | 9 | Israel |
| 10 | 10 | Sweden |
Why does it matter if older Americans have a relatively high disease burden? As the United States confronts coronavirus, the older population’s level of age-related disease and disability may affect the proportion of older adults who becomes critically ill. Individuals with underlying health conditions are more likely to have severe reactions to the COVID-19 infection, according to the CDC.
Cardiovascular diseases and cancers make up half of the age-related disease burden worldwide, according to Angela Y. Chang, assistant professor at the Danish Institute for Advance Study, who led the research team as a postdoctoral fellow at the University of Washington. Diabetes and chronic obstructive pulmonary disease (COPD, a respiratory disease) are also leading sources of disease and premature death, driving differences among countries.
“Italy’s adults have a relatively lower burden of diseases that we think are related to aging than people in other countries,” she said (see figure). Italy’s population, however, has a larger share of older adults than most other countries, which increases the overall level of age-related diseases, she noted.
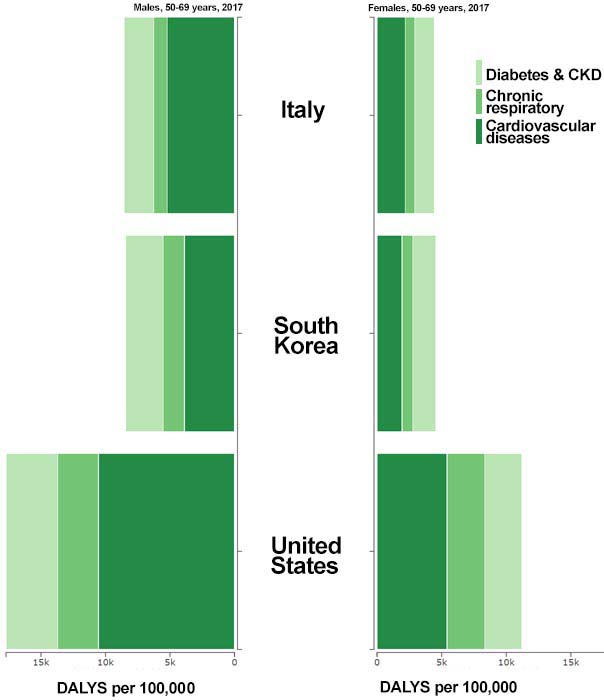
Note: Disease burden rate is based on the level of disability-adjusted life years (DALYS; healthy years lost) per 100,000 adults. CKD is an acronym for chronic kidney disease.
Source: Institute for Health Metrics and Evaluation, University of Washington, Global Burden of Disease Study 2017.
Supported by the U.S. National Institute on Aging, the study examined the level of age-related burden resulting from 92 diseases and conditions. Researchers used a measure that quantifies premature death and years of life lived in less than full health (disability-adjusted life years, known as DALYS) to calculate the age-related disease burden for each country.
This study is the first of its kind to explore both chronological age and the pace at which aging contributes to health deterioration, using estimates from the 2017 Global Burden of Disease study.
It identified wide variation in how well or poorly people age, showing that a 30-year gap separates countries with the highest and lowest ages at which people experience the health problems of an average 65-year-old worldwide.
Chang and colleagues report that 76-year-olds in Japan and 46-year-olds in Papua New Guinea have the same level of age-related health problems as an average 65-year-old. Americans at age 69, United Kingdom residents at 71, and Italians at age 75 have the same level of age-related health problems as an average 65-year-old globally.

The ENGAGE presentation demonstrates how faith communities and young people in the Sahel can work together to advance the future of the region by promoting a frank and open dialogue, and first and foremost, encouraging social tolerance. It underscores how religious leaders can use their influence in positive ways to condemn the practices of child marriage and female genital mutilation. The presentation also reinforces the message that religious leaders from the region are ready to encourage family planning use among young married couples and support family life education programs in communities.
The Sahel Faith ENGAGE initiative builds on the efforts of the PACE project to support policy dialogue about faith and family planning. Targeting three countries: Guinea, Mali, and Mauritania, the current activity brought together a task force composed of religious leaders (Muslim and Christian), youth, and government representatives to develop a multimedia presentation to promote dialogue about religion and young people’s reproductive health in the Sahel region.
Through this partnership and the presentation, PACE seeks to catalyze regional and national dialogue on the positive intersections of faith and young people’s reproductive health and development needs.
The ENGAGE presentation was launched on Dec. 4, 2019 at the 8th Annual Meeting of the Ouagadougou Partnership, in Cotonou, Benin. In coming months, it will be disseminated nationally and subnationally in the three target countries.
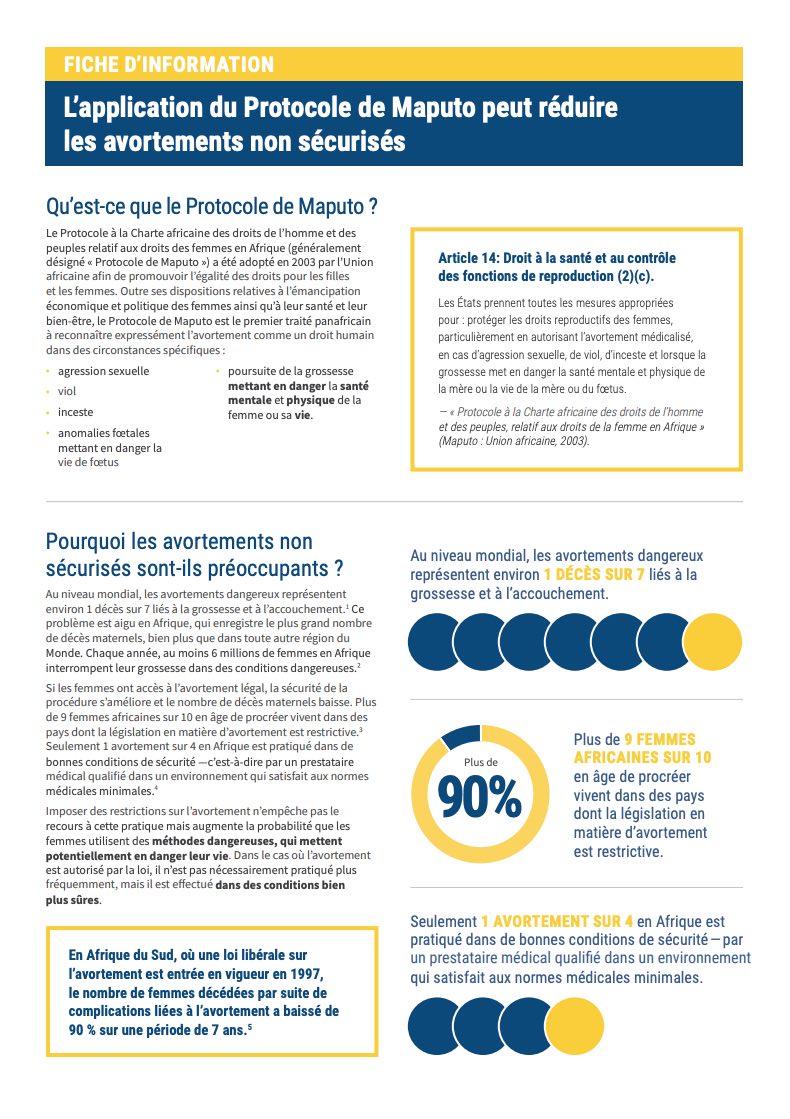
Le Protocole de Maputo, adopté en 2003, constitue l’un des premiers cadres juridiques pour la protection des droits et des libertés des femmes et des jeunes filles en Afrique.
Malgré des progrès, sa mise en œuvre reste difficile, puisque neuf femmes africaines sur dix en âge de procréer vivent dans des pays dotés de lois restrictives concernant l’avortement.
Le PRB a développé cette fiche d’information en tant qu’outil permettant aux décideurs, aux experts médicaux et juridiques ainsi qu’aux défenseurs de communiquer sur les avantages du Protocole de Maputo, dans le cadre du mécanisme de réponse rapide SAFE ENGAGE. La fiche d’information se concentre sur l’article 14 du protocole, qui met en avant la santé et « les droits reproductifs des femmes en autorisant l’avortement médicamenteux en cas d’agression sexuelle, de viol, d’inceste et lorsque la poursuite de la grossesse compromet la santé mentale et physique de la mère ou du fœtus ». Cette fiche utilise des données et des éléments visuels pour expliquer comment ce protocole peut réduire le nombre d’avortements non médicalisés.

In May, Linda Jacobsen, Lillian Kilduff and I helped organize a conference for nearly 300 American Community Survey (ACS) data users. This is the fourth ACS conference PRB has organized in partnership with the U.S. Census Bureau since 2014. If you missed the conference this year, don’t worry. We posted PDF versions of the conference presentations and recordings of the plenary sessions on the conference website.
Organizing a conference is kind of like organizing a wedding. It involves a lot of preparation, and when the big day finally arrives, you spend a lot time making sure everything is running smoothly. But now that a few weeks have passed, I wanted to take a step back and summarize some of my key takeaways from the event.
The conference began with some Census Bureau updates on ACS activities and operations. Steven Dillingham, the Census Bureau Director, expressed the importance the ACS and said “data users are the key to the continuous improvement” of the flagship survey. Regarding the 2020 Census: Dr. Dillingham said operations are on track, but with more than 26,000 distinct activities, there is still a lot of work to be done.

Steven Dillingham, Director, U.S. Census Bureau
Jim Treat (Assistant Director for Decennial Census Programs) announced the 2018 ACS data release schedule, which has shifted because of the lapse in federal funding earlier this year. He also provided high-level updates on several ACS Program activities, including a recent Workshop on Improving the American Community Survey, the new data.census.gov platform, efforts to ensure respondent confidentiality, and updated ACS Data User Handbooks, which include detailed case studies on how ACS data are being used for decisionmaking.
Next, Jennifer Ortman (Assistant Division Chief for Survey Methods and Measures in the American Community Survey Office) summarized the Census Bureau’s ongoing efforts to ensure the quality of ACS data. These efforts include changes to the 2019 ACS questionnaire and plans to use administrative records to reduce respondent burden, increase data reliability, and reduce costs.
The plenary session on Day 2 began with a Census Bureau update on new “disclosure avoidance” methods that could have long-lasting implications for ACS data users. As computational power has grown, privacy concerns and the risk of someone “re-identifying” ACS respondents has also increased.
Rolando Rodríguez (Research Mathematical Statistician at the Census Bureau) described the Census Bureau’s preliminary plans to ensure respondent confidentiality in the ACS. The bottom line is that the ACS will transition to formal privacy methods, but the Census Bureau is currently focused on protecting confidentiality in 2020 Census data, and it’s too early to say exactly how ACS data might be affected by new disclosure avoidance methods.
The formal privacy methods developed for the 2020 Census will inform ACS methods, but the ACS has additional features—more topic areas, complex survey design and survey weights, and population controls—that need more research. Once developed, the methods will be used to balance data privacy and data accuracy in the ACS data. For now, the Census Bureau plans to release the “standard complement of ACS tables and public-use microdata (PUMS) for 2018,” but is exploring the possibility of expanding the use of synthetic data to protect the PUMS data. Rolando also emphasized the Census Bureau’s commitment to data user involvement and feedback as these new formal privacy methods are adopted for the ACS.
Zach Whitman (Chief Data Officer at the Census Bureau) began his presentation with this chart, which shows the complex web of data tools currently available through the Census Bureau’s website.
This “forest of applications” is being replaced with a more centralized system (data.census.gov) designed to simplify access to Census Bureau data, including ACS estimates. What does this mean for ACS data users? Starting in June 2019, there will be no new data releases in American FactFinder (AFF). Zach encouraged data users to visit the new site and provide feedback: What you like and don’t like, and what changes you would like to see in future iterations (Email: cedsci.feedback@census.gov).
In her remarks, Connie Citro (Senior Scholar at the Committee on National Statistics) applauded the Census Bureau’s efforts to invite input from ACS data users but encouraged more “systematic, two-way interaction” between data users and Census Bureau staff “to best ensure that new privacy protection techniques and the new platform are implemented with full consideration of alternatives and user needs.”
The plenary sessions focused on informing data users about Census Bureau activities, but the main purpose of the conference was to showcase the work of ACS data users. The program included more than 50 presentations from data users representing a broad range of government agencies, academic institutions, and private-sector organizations.
Breakout session topics included:
During lunch on the first day, many ACS data users participated in informal meetups to discuss various topics and issues related to ACS data, including:
And during lunch on the second day, Census Bureau staff were on hand to lead product demonstrations and topical roundtables:
I want to thank all of the data users and Census Bureau staff who attended the 2019 conference, presented their work, and posted conference updates on Twitter.
A special thanks to members of our ACS Steering Committee and our Census Bureau partners for their help in organizing the conference. Their behind-the-scenes efforts were critical to the success of the event.
Zika is a mosquito-borne virus with no vaccine that is mostly spread by the bite of an infected Aedes mosquito. It can also be passed from a pregnant woman to her unborn baby, causing a unique pattern of birth defects. Viruses such as dengue and chikungunya are also transmitted by the same species of mosquito as Zika.
Based on work by Breakthrough ACTION + RESEARCH, this interactive online guide and video present seven behaviors that have the greatest potential to prevent transmission of the Zika virus and therefore Congenital Zika Syndrome. It is designed for program planners and implementers working on Zika response programs, with a focus on ensuring healthy pregnancies and births. Since the behaviors that reduce the mosquito population or prevent them from biting can also help prevent other Aedes-related viruses, this guide can also be used by those working to prevent dengue and chikungunya.
For each behavior, the guide explains key facts, instructs how to do the behavior correctly, provides tips for promoting the behavior, and offers supporting evidence. The guide includes a short video that can be downloaded and used for training or orientation, and downloadable PDF files for each behavior that can be printed and/or used for reference.
The guide is designed for program planners and implementers working on Zika response programs in Latin America and the Caribbean, with a focus on ensuring healthy pregnancies and births.
INTERACTIVE GUIDE TO PREVENT ZIKA
Comportamientos efectivos para prevenir el Zik
Family Planning High Impact Practices (HIPs) are a set of evidence-based practices developed by experts in the family planning sector that improve family planning and reproductive health outcomes. This webinar, hosted by the PACE (Policy, Advocacy, and Communication Enhanced for Population and Reproductive Health) project and the Implementing Best Practices Initiative Secretariat, explores how HIPs can be applied in development programs that integrate multiple sectors at the community level, including family planning.
The newly published web feature and policy brief, provides background on HIPs and explores the promising opportunity to expand their use within population, health, and environment (PHE) projects. Speakers Laura Cooper Hall (Population Reference Bureau), Caitlin Thistle (United States Agency for International Development), and Yvette Ribaira (JSI Research & Training Institute, Inc.) discuss the value of HIPs to PHE projects and family planning outcomes and highlight how PHE projects are already implementing HIPs elements in their activities.
The webinar concludes with a Q&A session between Caitlin Thistle, a HIP expert, and Yvette Ribaira, a PHE project implementer.
 ">
">

