Mark Mather
Associate Vice President, U.S. Programs


Associate Vice President, U.S. Programs

Senior Program Director

Senior Vice President, Programs
On December 17, 2025, PRB convened a small group of researchers, advocates, and policy experts to discuss factors that could impact the count of young children in the 2030 Census and the role research can play in addressing those risks. The goal was to identify shared priorities and areas where additional evidence could inform planning decisions in the years leading up to 2030.
Accurate census counts of young children matter. An undercount of young children in the decennial census means fewer resources for early childhood programs, reduced political representation for communities with young families, and flawed data for policy decisions that affect children’s health, education, and well-being. Young children, particularly infants and toddlers, have historically been undercounted at higher rates than any other age group, and the 2030 Census faces operational and budgetary constraints that could worsen this problem.
Addressing these challenges will require sustained investment in targeted research. This convening identified critical evidence gaps and outlined a research agenda designed to inform census planning and improve outcomes for children. However, translating this agenda into action depends on funders recognizing the urgency of this issue and committing resources to support timely, rigorous research in the years ahead.
This document is intended as a starting point for collaboration and a foundation for a shared research agenda focused on ensuring that young children are fully counted in the 2030 Census.
Participants agreed that the 2030 Census will be conducted under greater constraints than recent decennial censuses. Greater reliance on administrative records and online responses, combined with reduced in-person field operations, introduce new efficiencies but also new risks. These changes are unfolding alongside persistent budget uncertainty, staffing challenges within the Census Bureau, and declining trust in government.
For young children, these constraints are especially consequential. Infants and toddlers are already among the hardest populations to count because they are more likely to live in complex households, experience housing instability, and lack consistent representation in administrative data systems. Operational and contextual pressures that reduce follow-up, limit outreach, or increase reliance on imperfect data sources could compound existing challenges and exacerbate longstanding undercounts of young children.
The expanded use of administrative records was a central theme in the discussion. Participants recognized the potential for administrative data, including state birth records, to help identify young children who might otherwise be missed. But participants also emphasized that administrative records vary widely in their usefulness for census purposes.
Some administrative records lack current or usable address information, limiting their value for highly mobile families, children in informal housing, or those with complex living arrangements. Other administrative records include address data but are missing important demographic characteristics for young children, like race and ethnicity.
Participants noted that experiences with administrative records differ across programs and states. In some contexts, address coverage is relatively strong, while in others it is incomplete or unreliable. This variation underscores the need for careful, evidence-based assessment rather than assumptions about administrative record quality.
Young children in lower-income families are more likely to be missed. These families are less likely to show up in some federal records, but more likely to be included in state programs, making it important to understand which data sources best capture these children.
A central issue is whether states will be willing to share administrative data for census purposes. Concerns about privacy, potential misuse, and loss of control over sensitive information are making some states reluctant to share their data.
Taken together, uneven data quality and state participation mean that greater reliance on administrative records—without careful testing and evaluation—could amplify existing gaps, disproportionately affect the count of young children, and worsen longstanding inequities in child coverage.
Despite technological and methodological advances, an accurate address list remains the foundation of a complete census. Participants raised concerns about the future effectiveness of the Local Update of Census Addresses (LUCA) operation, which relies on state, local, and tribal governments to help identify missing or incorrect addresses, amid growing resource constraints.
When administrative records are available and of sufficient quality, they can help compensate for some address gaps—particularly for households connected to government programs. However, participants emphasized that administrative records cannot fully substitute for a complete and accurate address list. Housing instability, the growth of informal and nontraditional housing arrangements, and reduced in-field address canvassing were all identified as risks that disproportionately affect young children.
Birth certificates are another resource for improving address coverage for infants, but these data are typically held at the state level. Participants noted that state willingness to share address data may be shaped by broader trust concerns and uncertainty about how federal agencies may use or protect those data.
Trust, fear, and participation continue to shape outcomes
Participants emphasized that trust in the census and in government more broadly remains a critical determinant of participation, especially in immigrant and marginalized communities. Even proposals that are unlikely to be implemented—such as adding immigration or citizenship status questions to the census—can influence perceptions and willingness to respond.
Heightened concerns about immigration enforcement and data misuse—combined with the growing visibility of administrative data use across government— may make some parents and other caregivers more hesitant to share their information with census enumerators. Fears that data could be used for harm—or shared across agencies in ways that affect immigration status, benefits, or surveillance—were seen as a growing barrier to full participation.
While differential privacy does not affect whether children are counted, participants highlighted its implications for how census data are used. Noise added to protect confidentiality can distort small-area counts of young children and other population subgroups, making it harder to identify local undercounts, evaluate interventions, and allocate resources. Participants agreed that research is needed to help data users interpret and responsibly apply these data for child-focused policy and funding decisions.
Across topics, participants identified a gap between descriptive knowledge and actionable evidence. While much is known about which children are missed and where undercounts occur, there is far less evidence explaining why omissions happen or which interventions are effective.
Specific gaps highlighted during the discussion included:
Participants emphasized that without addressing these gaps, the field risks repeating past analyses without changing outcomes.
Participants noted that research on the undercount of young children has often depended on the efforts of individual Census Bureau staff or small teams, rather than being embedded as a sustained, agency-wide research priority. As a result, testing and evaluation related to young children has been uneven and vulnerable to shifting operational demands.
Based on the discussion, participants coalesced around a research strategy guided by three principles:
Participants identified the need for research that goes beyond demographic correlates to examine the mechanisms driving child omissions. This includes qualitative and mixed-methods studies exploring why some parents and caregivers aren’t reporting young children in the census, how household dynamics affect reporting, and how privacy and trust concerns shape responses.
Given the central role administrative records are expected to play in 2030, participants called for rigorous assessment of these data sources for young children. Priority areas include understanding gaps in coverage for infants and young children, exploring state-level differences in administrative data accuracy and program participation, and modeling the effects of reduced data sharing.
Simulation and scenario analyses were highlighted as especially useful because they allow researchers to test “what-if” scenarios—such as reduced field capacity or uneven access to administrative data—and assess how those conditions might affect the count of young children.
Research is needed to assess risks to address coverage, including the effectiveness of LUCA participation under constrained budgets and the impact of growing housing instability on census coverage for children.
Participants emphasized the need for updated research on trust, fear, and willingness to participate in the census. This research should account for the broader policy and enforcement environment, the increasing visibility of administrative data use, and the need to identify strategies that can reduce fear and rebuild trust among parents and other caregivers.
A consistent theme was the need to move from documenting problems to testing solutions. Participants emphasized a staged approach that identifies promising interventions, tests them using available data or experimental designs where possible, and translates findings into actionable guidance.
Finally, participants stressed that research must be communicated in ways that resonate with policymakers, funders, and community leaders. Linking census accuracy for young children to funding, services, and long-term outcomes was seen as essential for sustaining attention and investment.
Several participants emphasized that improving the Census Bureau’s population estimates of children—both within and outside the decennial census—could have benefits well beyond 2030. Stronger child population estimates would improve the Bureau’s ability to target census operations, assess coverage through demographic analysis, and support federal funding formulas and survey controls throughout the decade. Participants noted that these improvements would remain critical even if the 2030 Census faces significant challenges, given the widespread reliance on population estimates across federal programs.
The December convening underscored both the urgency and the opportunity facing the research community. Without targeted, coordinated research, longstanding challenges in counting young children are likely to persist into 2030. At the same time, the period leading up to the next census offers a window of opportunity to generate evidence that can shape decisions and improve outcomes.
The research community cannot do this work alone. Funders have a critical role to play in supporting the timely, rigorous research needed to improve child coverage in 2030. Strategic investments now—in qualitative studies, administrative data evaluation, and intervention testing—can yield measurable improvements in how young children are counted and, ultimately, in the resources and services that reach them. The window for impact is closing, and sustained funding commitment is essential to translate this research agenda into meaningful change.
Funding for this work was provided by the Annie E. Casey Foundation. The views expressed in this article do not necessarily reflect the views of the Foundation.

The Voice for Data
In 2024, population aging and low fertility caught the world’s attention. Long predicted by demographers, these trends worked their way into the popular discourse—grabbing headlines, sparking debates, and filling PRB’s inboxes with questions from media, researchers, and the public.
These issues are complex, consequential, and real—yet, too often, they are reduced to alarmist coverage that obscures more than it reveals. At PRB, we believe that rigorous data and thoughtful analysis are essential to moving beyond headlines toward understanding and progress. Our mission—to use population data to help solve pressing societal challenges—has never been more critical.
To that end, we’re leaning into the evidence and making sure the insights they provide are widely—and freely—available, tempering those alarmist headlines with evidence-based context. It’s what we do so well here at PRB, and we know our work is vital to helping stakeholders understand many of the world’s most-pressing challenges.
Does every generation in the United States still do better than the last? What’s the economic value of unpaid care work? Is there really a population crisis because of low fertility? How can we prepare to meet the needs of aging populations? These are just some of the questions we addressed in Fiscal Year 2024.
Staff dug into the data and analyzed the impacts and implications of demographic changes in the United States and abroad. They also partnered with peers at organizations from around the world—from UNFPA Asia in Bangkok, Thailand, to the CREG Center in Theis, Senegal—to share findings with a global audience.
It was a year of speaking up and cutting through the noise with evidence. Every time. Accurate data and research are essential to our understanding of population dynamics and to crafting effective solutions to issues affecting people’s health and well-being.
My heartfelt thanks to all of you who supported our work this past year by attending a webinar, reading a report, sharing a post, funding a program, or donating a dollar. You helped us speak up as a voice for data in FY2024.
Sincerely,
![]()

President and CEO
“A young woman in the U.S. today, between the ages of 25 and 34, is more likely to die than at any point since at least the 1960s,” reports Sara Srygley, research associate at PRB.
“We’ve seen that young women today are doing many of the things they’ve been promised would lead to a better life, and these are things that worked in the past,” Srygley says. “Yet our research shows that despite their best efforts, they still face very real challenges compared with previous generations in some of the most fundamental areas of life.”
PRB’s original analysis of young women’s well-being shows that Millennial women ages 25 to 34 are doing worse on critical health and safety measures than women of the same ages from the Generation X and the Baby Boom generations. Today’s young women are more likely to die from preventable causes, be murdered, or die by suicide. These risks are even more pronounced for pregnant women.
A society is only as healthy its people are. Today’s young women face an uncertain future, marked by the erosion of rights and protections, complicated economic reality, and mental health tolls from the political, ecological, and social climates.
“How we address these threats to Millennial women’s well-being will set the stage for how Gen Z fares as they reach their young adulthood,” Srygley says.
PRB’s “Losing More Ground” report drove dialogue with experts and the media on poor state of women’s well-being in the United States. The findings reached more than 3 million people across print and digital media platforms, including coverage by CNN, ABC News, Axios, and Forbes.
We also partnered with The Center for Law and Social Policy, Justice and Joy National Collaborative, and Young Invincibles for a public discussion of the implications and potential policy solutions that would drive better outcomes for young Americans.
“We need to go beyond meeting just basic needs and try to build a system of benefits that is designed for people to thrive and experience abundance,” says Cara Brumfield, then a director at The Center for Law and Social Policy.
You can read the full report or hear from experts about why our findings matter.
“Since the 1960s, world population has more than doubled, but the growth rate has been falling the entire time,” says PRB’s Jennifer D. Sciubba in her TED Talk. “We’re witnessing the most fundamental shift to take place in modern human history.”
Two out of every three people in the world live somewhere with below replacement-level fertility (2.1 children per woman). From Canada to France to Japan to Türkiye, people are choosing to have fewer—or no—babies. And while fewer babies are being born, more people are living longer. China’s population aged 65 and older is expected to increase 85% by 2050.
“A country like the United States with low fertility—a shrinking and aging population—has dramatic implications, affecting everything from the health care workforce to transportation infrastructure,” says Beth Jarosz, Senior Program Director at PRB.
“People are the foundation of a society,” adds Sciubba. “We’re the workers and the voters and the soldiers and the caregivers. So, how many of us there are and who we are, that matters. We’re on track for there to be more people over age 60 than under the age of 14 by the middle of this century.”
A large older adult population will likely face challenges with financial stability, health, and caregiving. If countries don’t adapt to meet this shift, their social and economic systems could become overloaded. Labor costs and inflation will increase, social security systems could go bankrupt, and older adults will face a greater risk of poverty. All of these factors will make it even more costly for people to have children. “The question many world leaders should now be asking is how to plan for the strain that an aging and shrinking society puts on the care economy and the workforce,” Sciubba says.
We brought together nearly 500 people from across the globe and experts from the Peace Research Institute Oslo and Institute for the Future to discuss strategies for building a more resilient world in the face of population aging. Together with the UNFPA Asia and the Pacific Regional Office, we also briefed the media on demographic changes in the region and how policies can help support thriving aging populations. And we dug into the latest research on healthy aging to create a report, with funding from the Coordinating Center for the Centers on the Demography and Economics of Aging and Alzheimer’s Disease and Alzheimer’s Related Dementias, to highlight the importance of social connections in healthy longevity.
Rebecca Shamash of the Institute for the Future talked about how today’s technological boom could lead to massive productivity gains: “And if that was something that we could harness to really set ourselves up for this future world,…how could we use this technology to get us there a little bit faster, and to help us create more comfortable lives in the future?”
Check out the PRB x TED event, get highlights from the media briefing, or read more about social connections and aging.
“Primary health care helps people live longer, healthier lives, but nearly 50% of people in the world today can’t access quality care,” says Toshiko Kaneda, Technical Director of Demographic Research at PRB. “This is a serious challenge, and it will become bigger as the older adult population grows.”
When people can access quality primary health care at every stage of their life, they’re healthier longer. A healthier population can have a huge impact on maternal mortality and the burden of chronic diseases such as hypertension and diabetes that are commonly seen at older ages. It also lessens the demand for caregiving.
Access to good primary health care is already difficult for people across the globe, particularly in low- and middle-income countries. Many governments don’t have sufficient resources to meet their populations’ basic health needs, and skilled health professionals are overworked due to staff shortages, impacting the quality of care.
“The current struggle to access quality health care, combined with the projected near doubling of the global share of the population ages 65 and older by 2050, means health system strains will intensify. If investments aren’t made to improve access to good primary health care, the situation will be much worse 25 years from now, and the demand for caregiving, both paid and unpaid, will skyrocket,” says Kaneda.
We shined a spotlight on primary health care in the 2024 World Population Data Sheet, produced under the USAID-funded PROPEL Health project. This year’s Data Sheet featured 10 special indicators that reveal health spending per capita, use of family planning methods, health care workers per 10,000 population, and the Universal Health Care service coverage index for more than 200 countries and territories. We also created a media brief that journalists can use as a primer when reporting on the topic.
In 2024, over 1.3 million people accessed the World Population Data Sheet online, and 45,000 people downloaded the poster to use in classrooms and workplaces. Users got an inside look at the strength of primary health care in their countries—and how it compares to the rest of the world.
“Health spending from all sources per capita (US$) is $1,260 for the world and $74 in India, the most populous nation in the world. How might low investment in health care across populous nations affect global priorities and change the ability of governments and multilateral organizations to respond to events such as pandemics, migration, and climate change?” we prompt in the media brief.
Explore the 2024 World Population Data Sheet or learn how to report on this topic.
“Every adult has engaged in some form of care work,” says Cathryn Streifel, Senior Program Director at PRB. “But because of the differing expectations of roles for men and women, which inform how our societies are structured, most of it is done by women and is unpaid. Globally, women perform 76% of unpaid care work.”
Care work—the tasks involved in supporting others’ needs related to age, disability, or illness—is essential for human well-being, for societies to function, and for sustainable economic growth. Unpaid care work results from a lack of public investment in care services and infrastructure, and it comes with many costs, including substantial economic loss for uncompensated labor. Around the world, women regularly forfeit education and work opportunities to do the essential work of caring for children, older adults, and other family and kin.
“Women in Francophone West and Central Africa do the majority of domestic work, also called family care, and it keeps them out of school and the formal workforce. Because this work is unpaid, it remains invisible in Gross Domestic Product and in analyses of economic progress,” says Aïssata Fall, Africa Director at PRB. “In Togo, unpaid domestic work represents an estimated US$2 billion in social capital. And 30% of this work is done by women.”
“The United States also faces a serious burden of unpaid care work,” adds Beth Jarosz, Senior Program Director at PRB. “And it can have significant negative economic consequences, especially when that work is unpaid or underpaid. Combined with complex social safety net programs, the caregiving burden can limit women’s career opportunities, reduce their earnings potential, and increase financial hardship for women and their families.”
We collaborated with the CREG Center in Theis, Senegal, to develop a guidebook to support evidence-based discussions about unpaid care work with policy audiences in Francophone West and Central Africa. The real-world examples developed with local context provide a vital resource specifically for Francophone audiences. In the United States, we teamed up with Jessica Calarco, sociologist and author of Holding It Together: How Women Became America’s Safety Net, to discuss the issue in the United States with an expert panel including prominent advocates and researchers.
“[Y]ou can’t actually DIY society,” says Calarco. “Essentially forcing people to manage all that risk on their own has left many American families and communities teetering on the edge of collapse. And yet, … we haven’t collapsed in part because we have disproportionately women been the ones who are holding it together, filling in the gaps in our economy and the gaps in our threadbare social safety net.”
“It is not enough to simply recognize unpaid care work. It is crucial to understand its nature, scale, and age- and gender-related dynamics,” says Fall. “Without this understanding, there are risks of misdirecting public policy—or even reinforcing inequalities. Unpaid care work represents a major source of national wealth and well-being, yet it remains largely underestimated in current analytical frameworks.”
Explore the resource guide on unpaid care work, watch the webinar on America’s safety net, or visit the blog for webinar highlights.
“Postpartum hemorrhage is the leading cause of maternal mortality across the world, which is astonishing because it’s largely preventable,” says Megan Ivankovich, head of the USAID-funded MOMENTUM Knowledge Accelerator project at PRB. “More than 90% of these deaths occur to women in low- and middle-income countries.”
Postpartum hemorrhage occurs when the mother experiences blood loss of 500 milliliters or more within 24 hours after birth, according to the international definition. That’s more than 16 ounces, or over half a liter. Each year, about 14 million women around the world suffer from postpartum hemorrhage—and 70,000 die.
“Despite postpartum hemorrhage needlessly stealing mothers away from their families, there’s no consistent data collection on the condition. In fact, there’s a lot of disagreement about the factors involved, from the amount of blood loss to clinical signs and symptoms,” says Ivankovich. “We’re missing critical evidence that could save lives.”
The Sustainable Development Goals aim to reduce maternal mortality to 70 deaths per 100,000 live births by 2030, but 2023’s rate of 197 deaths starkly demonstrates that the world has a long way to go to reach this target. Around 70% of maternal deaths occurred in sub-Saharan Africa, and about 17% occurred in southern Asia, reports the World Health Organization.
We organized a webinar and two studies under USAID MOMENTUM to share guidance and tools with officials in health care and government and other health practitioners on the use of medications that aid uterine contractions and reduce postpartum hemorrhage but can also harm mother and baby. PRB project staff shared research, tools, and learning with 233 participants from 64 low- and middle-income countries on how to safely use these medications, called uterotonics.
“The webinar [was] a practical session with evidence relevant to the settings in which I am operating, and the operational research can be adapted,” says one participant from Kenya Amref Health Africa. Another participant from Cambodia shares that they “could use [the information] as an up-to-date resource to support the Midwifery Curriculum update in Cambodia.”
Our activities helped inform the uterotonics agenda for India’s Ministry of Health and Family Welfare and the Federation of Obstetric and Gynecologic Societies of India, who are developing enhanced guidelines on uterotonic use.
Learn more about uterotonics.
“There are too few young Americans and future workers being born to replace retirees,” says Diana Elliott, PRB’s Senior Vice President of Programs.
The United States had 1.4 million fewer workers than jobs in 2024. The absence of so many people from the workforce significantly impacts tax structures, distribution of tax burden, ability to repay debt, and GDP, as well as population dynamics.
The United States is confronting a demographic future of fewer workers while its population ages 65 and older grows rapidly. At the same time, changes in mortality and illness may be contributing to long-term labor force challenges. Policymakers can intervene to better engage workers who have been sidelined, such as people with disabilities and families with young children; support a wider variety of educational paths for employment; and evaluate wages and regulations.
“In the news, you may hear complaints about how young people aren’t working,” Elliott says. “In fact, there just aren’t as many young people to fill roles, which makes workforce training programs all the more important in the larger U.S. context.”
We got together with the Critical Labor Coalition and former U.S. Secretary of Labor Alexander Acosta for an open exchange about what the latest workforce data mean and how they could be used to develop short- and long-term responses to meet the challenge—individuals from over 40 countries joined in to ask questions and share ideas. And we spoke with media like The New York Times about the demographic factors involved in the U.S. labor shortage.
“Do we really treat all tracks equally and say, is the goal a family-sustaining wage, or have we started biasing the conversation in favor of those that have our backgrounds?” asks Secretary Acosta. “All of us on this talk on this panel went to college … if you look at the labor force data, you see that the biggest declines are not among the college graduates, but among those that didn’t go to college. And what are we doing to address them?”
“Accurate population data are critical for understanding our communities and planning for the future. So when decisionmakers can’t get the data they need, plans can miss the mark—with serious consequences,” says Mark Mather, Associate Vice President of U.S. Programs at PRB.
The U.S. Census Bureau collects and publishes vast amounts of data on the country’s population characteristics through the decennial census and the American Community Survey, but these raw data can be difficult to use. The Census Bureau also isn’t always informed on what data users need to know about the data to meet their communities’ needs.
“If decisionmakers and planners can’t track social and economic change where they live—things like workforce development, health insurance coverage, and child poverty and well-being—they can’t support people as their needs change,” says Mather. “A strong data infrastructure is critical to sustaining a healthy society.”
Comprehensive population data can help data users and others in government, business, academia, and nonprofits better understand and support their communities.
We teamed up with the U.S. Census Bureau and the Southern California Association of Governments to share resources, tools, and shortcuts with hundreds of data users across the United States. We met people in their communities, working with the University of Utah, Texas Demographic Center, the New York Law School, and the New York City Department of City Planning to host “ACS on the Road” events in Salt Lake City, Austin, and New York . With these tools at hand, they can more easily access and use U.S. population data in the American Community Survey (ACS) and better serve their communities’ needs.
“Are you finding that the data you need are not published in these estimates? … What do the data look like on a daily basis? And finally, with the tool or tools you are using, what limitations do you face accessing ACS data?” asks Mary Ana McKay, survey statistician in the American Community Survey Office. “These questions might have different answers depending on the day or the data you need.”
Which tool to use, she says, is “all about the best way to address your needs.”
Get tips on ACS data resources and discover data users’ needs.
“If countries are to make the most of their annual budgets, they need to have a clear understanding of how their investments performed in the past and of current and expected population needs. So, data collection, data analysis, and transparency of the budgeting process are key factors in developing effective public budgets,” says Reena Atuma, Activity Manager for this work at PRB.
Where these elements are lacking, the health of societies may suffer as some budgets fall short of demands, and services and infrastructure struggle to meet community needs. Researchers and decisionmakers may refer to analysis of past budget performance, tools for demographic dividend-sensitive budgeting, and census data to effectively support their communities.
“The labor, time and cost required to conduct a population census and analyze the data are significant,” says Jennifer D. Sciubba, President of PRB. “When countries can’t complete the process, their policies and programs may not be as effective as they could be.”
Accurate and transparent data help countries track needs and decide where to direct limited resources for the greatest impact. Prof. Latif Dramani, President and Coordinator at the CREG Center, notes in our joint webinar that this often means prioritizing strategic investments in human capital—education and health—over the operational costs of government institutions.
Without proper analysis, countries may make more investments in sustaining governing structures rather than in developing economic ones. “So these countries cannot stand up on their own feet until they can really fix this issue and balance out the structure,” Prof. Dramani says.
We collaborated with the Union for African Population Studies (UAPS) on a report that spotlights how researchers across Africa are using census data in development planning. We also worked closely with civil society organizations, local government officials, and others on subnational health financing challenges and solutions in Kenya. This financing work is part of a larger effort across the continent to boost the capacity of local civil society organizations to advocate for and ensure accountability in health financing.
Together with CREG, we brought experts, parliamentarians, and ministers together in West Africa to discuss tools that help countries harness the demographic dividend through budgeting. Our combined efforts opened high-level political dialogue between policymakers, ministry technical staff, and civil society on how age and sex shape people’s ability to fully participate in economic growth. This dialogue aligns with ongoing efforts to integrate unpaid care work into public policies.
“The [demographic dividend sensitive budgeting, BSDD] framework had influenced national strategies and opened dialogues between ministries, parliamentarians, and civil society,” says Astou Diouf, Director of Gender Equity in Senegal’s Ministry of Women, Family, Gender, and Child Protection. “These studies have enabled us to make recommendations to decisionmakers before the budgeting and point out priority for action.”
“[T]he results that have been shown by the scientific research show us that BSDD can really benefit us in taking advantage of the demographic dividend,” says Dr. Larba Issa Kobyagda, Director General of Economy and Planning, Ministry of Economy, Finance, and Development in Burkina Faso. “… [W]e must work so that the results of this research do not remain disconnected from policies, from politics.”
Explore how census data are used across Africa; hear more about budgeting processes for a demographic dividend; watch the webinar on strengthening budget systems in Africa; and read about domestic health financing in Kenya.
Webinar: Where Is the Workforce? Understanding the U.S. Labor Shortage and Working Toward Solutions
College Degrees Yield Lifetime Benefits for Disadvantaged Students
Five U.S. Facts and Trends in 2023 That You Should Know
Population Bulletin: Census Across Africa: Using Census Data for Policy and Planning
Should We Despair Over the Demographic Divide?
3 Bright Spots for Rural Appalachia—and 3 Struggles Compared to the Rest of Rural America
How Can Korea Respond to Its Population Crisis?
PRB Africa Highlights the Importance of Youth in Sustainable Development Work
PRB and CREG Share Tools for Capturing the Demographic Dividend in Senegal
PRB and Population Association of America Brief Congress on Maternal Death Crisis
A Patchwork of Access: Self-Managed Medication Abortion in Post-Roe America
PRB Kenya Presents at Nairobi Health Financing Conference
Race/Ethnicity Categories in Federal Surveys Are Changing: Implications for Data Users
Inaugural ACS on the Road Event Connects Texas Data Users With Census Bureau Staff
American Community Survey Resources, Shortcuts, and Tools Workshop
RTAC Partners Share End-of-Project Accomplishments and Impacts
The False Narrative of an Africa Unscathed by COVID-19
Citizenship, Ancestry May Help Determine Who Gets the ‘Hispanic Health Advantage’
College Shapes Black, White, and Latina Women’s Work and Family Lives Differently
Crowded Coasts Put 1 in 10 Americans at Risk for Floods, Other Hazards
Webinar: Writing About Population Research for Non-Scientists
From Paper to Practice: How PRB Supports Researchers to Put Their Results Into Action
Rural America Is Aging—Without Enough Care Workers
Webinar: How Women Became America’s Safety Net
Why Better Care Policies Matter for Gender Equality and the Economy
In Togo, PRB and CREG Discuss Importance of Recognizing Unpaid Care Work With Women Leaders
Fact Sheet: Aging in the United States
More Than Shelter: How Housing Affordability Is Linked to Older Americans’ Health
New Biomarker Research Provides Insights Into What Speeds up or Slows Down the Aging Process
No Matter Where They Lived, Older Americans With Dementia Were More Likely to Die From COVID-19
10 Things to Know About Older Americans’ Mental Health During the Pandemic
Safer but Alone: How COVID-19 Protections Affected Older Adults’ Mental Health
A Shift in Hunger: U.S. Food Policy and What We Learned From the Pandemic
In the Nest: Did the Pandemic Push More Young Adults to Live With Their Parents?
Is Your Child Misbehaving? Try Reasoning With Them
The Rise of the No-Bachelor’s Bachelor?
Expanded SNAP Benefits Boosted Food Security During the COVID-19 Emergency, Study Finds
![]()
The generous support we receive from organizations and individuals helps make our work possible. Thank you.
PRB worked alongside 15 organizations in 2024.
Through their generous contributions, the individuals listed here made it possible for PRB to fund essential program expansion and organizational innovations during the fiscal year ending Sept. 30, 2024.


Senior Technical Director
Today, an estimated 7.2 million Americans ages 65 and older live with dementia. While conversations around dementia often evoke nursing homes, most older Americans living with dementia are actually aging in place in their homes. Home-based care has become more common over the last decade, partly because it is more affordable and aligns with what many people prefer.
People living with dementia often face both medical and practical barriers to obtaining care, including challenges with memory, decision-making, and mobility. These difficulties make access to effective care at home not just helpful but essential to supporting their ability to remain safely in the community.
Despite its benefits, home-based care is not without challenges, including the financial burden of paying out-of-pocket for services not covered by Medicare and Medicaid and the emotional toll on family members who often take on day-to-day caregiving responsibilities. Understanding how home-based care works for the growing population of older adults with dementia is critical for improving how dementia is managed in the community and providing better support for older adults and their families.
Home-based care typically falls into two categories: home health care and home care. Home health care refers to medical services provided by licensed professionals, including skilled nursing care, physical therapy, and medical social services. It is covered by Medicare if prescribed by a doctor or nurse practitioner. Home care refers to non-medical services to assist with housekeeping and the activities of daily living, such as bathing and dressing. Medicare does not cover home care unless it is provided with medical care, but Medicaid covers home care in some states.
Based on data from the Health and Retirement Study (HRS) and Medicare claims between 2012 and 2018, Julia Burgdorf and her colleagues found that approximately 30% of home health care users had a dementia diagnosis.1 Older adults with dementia were twice as likely to use home health care compared to those without dementia.
About half of those with dementia were referred to home health care without a preceding hospitalization, compared to slightly less than a third of those without dementia. This finding highlights the importance of home health care as a key source of clinical care for older adults with dementia, not just for recovery care, Burgdorf and her colleagues said.
Once enrolled in home health care, people with dementia received care more times (an average of 1.4 times compared to 1 time) and for longer periods (median of 56 versus 40 days) than people without dementia. They were also more likely to receive personal care, medical social work, and speech-language pathology services than those without dementia.
However, among people who received services, those with dementia had fewer visits for skilled nursing and physical therapy, the researchers found.
“Existing prospective payment structures incentivize HHC providers to limit the number of visits in order to lower costs and maximize profits,” they wrote. And “the 2020 implementation of a new Medicare HHC payment model, the Patient-Driven Groupings Model (PDGM), may further incentivize limiting visits for people living with dementia.”
The new payment model aims to reimburse providers based on how sick patients are—but it doesn’t directly account for dementia status, Burgdorf and team note. It also reduces reimbursement for community referrals, though many people with dementia enter care this way. Differences in coverage between Medicare Advantage (private plans) and fee-for-service (the traditional government-run plan), along with workforce shortages and fragmented care systems, may create additional barriers for people with dementia, they explain.
Burgdorf and colleagues suggest several ways to improve home health care for people with dementia, including:
Many older adults end up paying for home care out of pocket because long-term care is not included in Medicare, Medicaid coverage is inconsistent across states, and few people have private long-term care insurance, according to another analysis.
“The financial burden of out-of-pocket payment for home care is significant, particularly among people with dementia and those with limited income and wealth,” conclude Karen Shen and colleagues, who used Health and Retirement Study (HRS) data (2002-2018) to measure the financial burden of home care.
Home care also often results in ongoing expenses over a long period of time, unlike most other health care costs, they found.
In recent years, people with dementia made up one-third of an estimated 3 million people who received home care and almost half (45%) of the over 600,000 people who paid for at least some of this care out of pocket, according to the researchers.2 Among those with dementia who paid out-of-pocket, half (51%) spent over $1,000 per month, compared to one-fourth (26%) of those without dementia. Additionally, people with dementia were much more likely to pay for full-time help, defined as 40 hours or more per week, compared to those without dementia (46% versus 22%).
Although higher-income individuals are more likely to pay out-of-pocket, many people with lower incomes also do so, largely because those with fewer financial resources are disproportionately affected by disability and dementia, the authors note. In fact, about half of those paying for home care out of pocket were poor or near-poor, defying the common perception that private home care is used only by individuals with higher incomes.
Those who are poor and have dementia experienced disproportionate financial burdens, as they spent 87% of their household income on home care, compared to 32% spent by their peers without dementia, and 22% spent by high-income individuals with dementia (See figure).
These findings suggest that those with dementia and limited financial resources may not be getting the care they need.
“Policies aimed at easing the financial burden of home care are essential, particularly for low-income individuals with dementia who experience the greatest financial burden,” argue Shen and her colleagues.
They recommend policies to reduce unmet care needs and financial hardship while also making the system more equitable and responsive to the realities of aging at home with dementia, including:
To make these programs financially sustainable, they recommend targeting benefits to the most vulnerable individuals and incorporating cost-sharing mechanisms so that those with more resources help shoulder the cost of care.
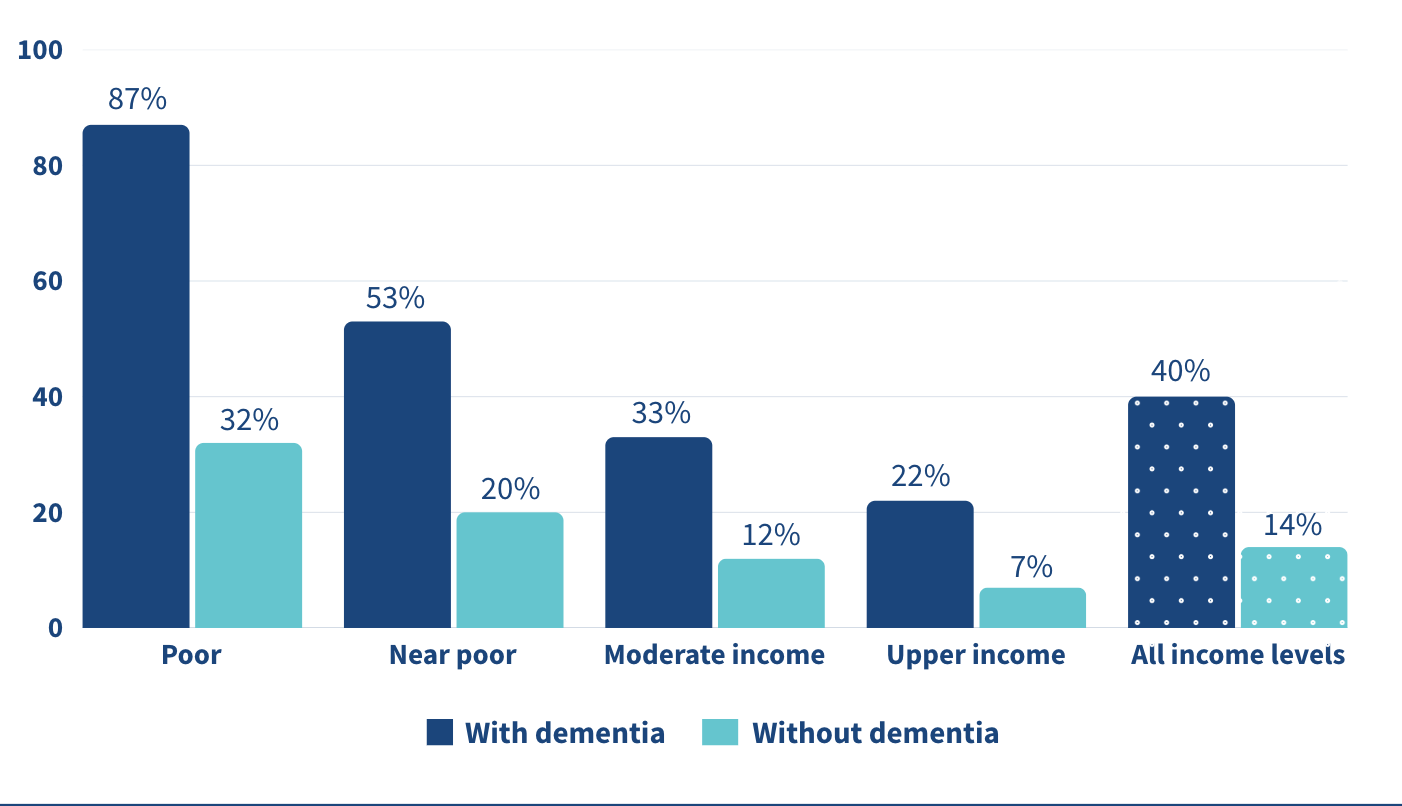
Note: “Poor”: 100% of the Federal Poverty Level (FPL); “Near-poor”: 100-200% of FPL; “Moderate-income”: 200-400% of FPL; and “Upper-income”: >400% of FPL.
Source: Karen Shen et al., “Paying for Home Care Out-of-Pocket Is Common and Costly Across the Income Spectrum Among Older Adults,” Health Affairs Scholar 3, no. 1 (2025).
Even with paid home care, most dementia care still falls on family and friends. In the United States, over 11 million unpaid caregivers provide over 15 billion hours of dementia care every year, according to Yeunkyung Kim and his colleagues.3 One way to give caregivers a break is through respite care—short-term care that lets family members step away for a few hours or days. Ultimately, respite care aims to help sustain caregiver health and delay the institutionalization of the people in their care.
Yet its use remains limited. Only 16% of Black caregivers used respite services compared to 32% of white caregivers in 2015, representing a significant gap of 12 percentage points, Kim and team found. Although this racial gap had been reduced or eliminated by 2017, respite care use remained low among both Black and white caregivers. Data are from the National Health and Aging Trends Study (NHATS) and the National Study of Caregiving (NSOC) from 2015, 2017, and 2021.
Even though there have been efforts to expand access, too many caregivers are still doing this difficult work without enough support. This highlights the persistence of structural and informational barriers to care—including financial cost, lack of awareness, cultural expectations, and insufficient supply of respite providers.
The underuse of respite care represents a missed opportunity to support the mental and physical health of caregivers, and thereby also the stability of dementia care at home.
Kim and colleagues recommend several strategies to improve access to respite care for families supporting older adults with dementia, including integrating respite services more fully into long-term care systems, particularly through expanded support in Medicaid-funded programs like home- and community-based services waivers.
Better outreach and clearer communication could also raise awareness of available services, since many caregivers remain uninformed or face fragmented information, the researchers note. There is a clear need for more flexible respite options that can accommodate the diverse cultural, financial, and scheduling needs of caregivers. For example, offering evening or weekend respite hours for those who work during the day, or providing in-home options for caregivers who are uncomfortable with facility-based care, could make a meaningful difference.
Simplifying program design, reducing waitlists, and ensuring consistent availability are also key to increasing use of these services, they said.
1. Julia G. Burgdorf et al., “Variation in Home Healthcare Use by Dementia Status Among a National Cohort of Older Adults,” The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences 79, no. 3 (2024).
2. Karen Shen et al., “Paying for Home Care Out-of-Pocket Is Common and Costly Across the Income Spectrum Among Older Adults,” Health Affairs Scholar 3, no. 1 (2025).
3. Yeunkyung Kim et al., “Trend in Respite Use by Race Among Caregivers for People Living With Dementia,” The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences 79, Supplement 1 (2024): S42-S49


Contributing Senior Writer
Associate Vice President, U.S. Programs
Early onset chronic disease, a growing caregiving gap, and climate change are among the major trends affecting the health and well-being of older Americans and their families, according to leading scholars from across the country.
Before a standing-room-only crowd at the 2025 meeting of the Population Association of America in Washington, D.C., experts identified seven key themes that are challenging policymakers, planners, and families as the U.S. population rapidly ages.
The United States has experienced the earliest and greatest slowdown in life expectancy improvements among higher-income countries, reported Eileen Crimmins of the University of Southern California/University of California-Los Angeles Center on Biodemography and Population Health.
“We have horrible life expectancy—and it’s getting worse and worse,” she said, pointing to the diverging line for the United States in Figure 1. Though premature deaths from heart disease and stroke have declined, Americans today are unhealthy for a longer portion of their lives, coping with chronic diseases and conditions such as diabetes, hypertension, arthritis, cancer, and heart problems.
While we “have a long way to go” to improve the health of the U.S. population, Crimmins said, new research into biomarkers gathered through blood and other medical tests is offering clues into what speeds up or slows down the aging process, including stress levels, income, and social connections over a lifetime.
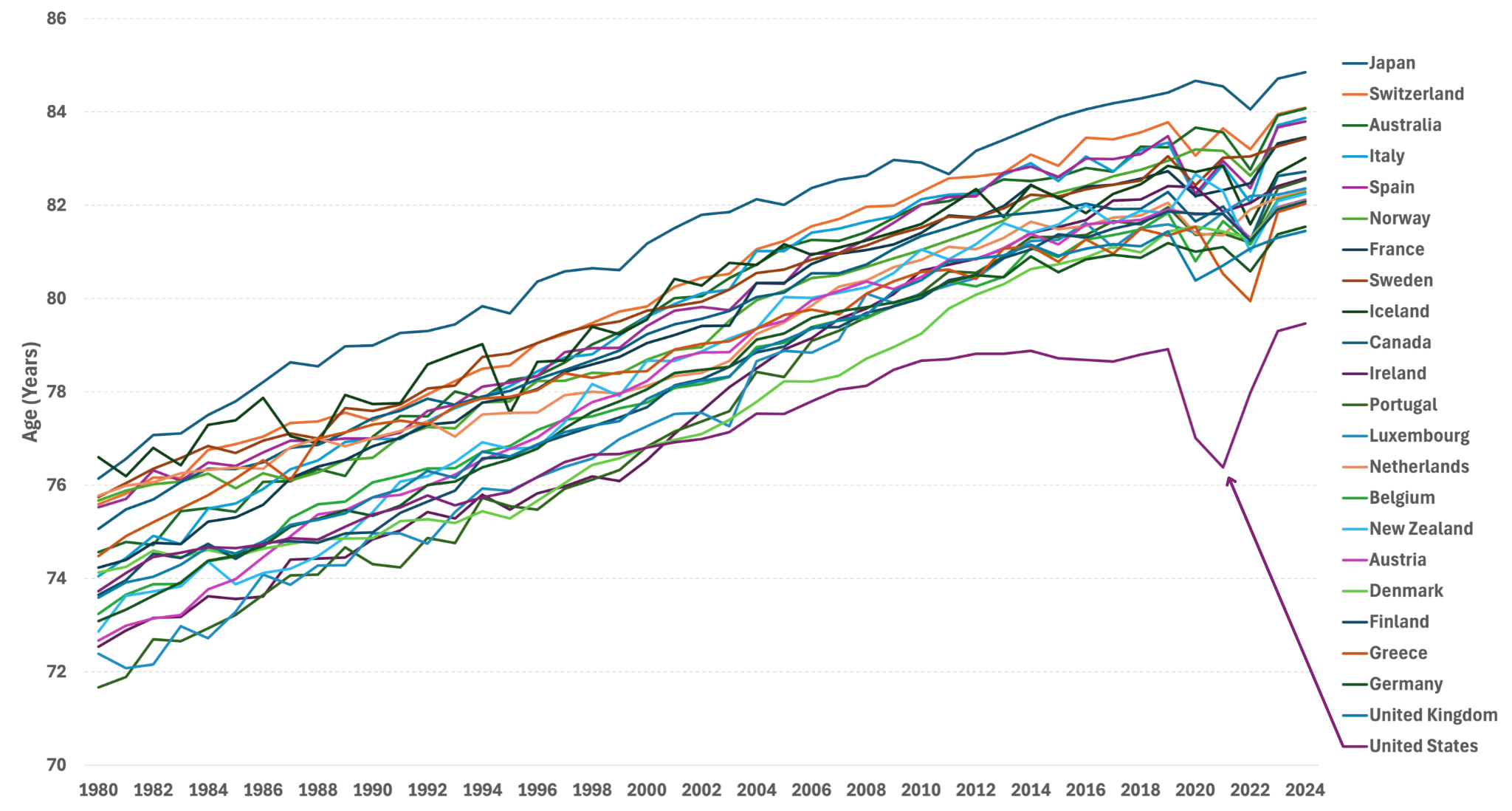
Source: United Nations, World Population Prospects.
While advances in health care have succeeded in preventing many early deaths, older people are spending more time living with chronic diseases today than two decades ago, Crimmins’ forthcoming research shows. Americans spent more years after age 65 living with diabetes, cancer, heart disease, arthritis, and high blood pressure in 2018 than in 1998, she has found.
Scott Lynch of the Duke Center for Population Health and Aging agrees. Over the past century, complex chronic conditions like cardiovascular disease and cancer have replaced infectious diseases like pneumonia and tuberculosis as the leading causes of death, he noted. In addition to biomarker research, longitudinal studies that follow individuals over decades have contributed to a growing understanding that events and conditions in childhood and adolescence shape health and lifespans in adulthood and old age, he said.
Improving the health of children and young people has profound effects later in life, argued William Dow of the Center on the Economics and Demography of Aging at the University of California, Berkeley. He pointed to new research showing that people with Medicaid insurance in childhood have better health as adults. “By reducing disability and keeping people in the labor force, Medicaid is actually paying for itself,” Dow said.
Family members provide most of the care that enables older people to live safely in their own homes, said V. Joseph Hotz of the Center for Healthy Aging Behaviors and Longitudinal Investigations at the University of Chicago. Among care recipients ages 65 and older, 69% receive only informal home care from friends and relatives, whereas just 5% receive only formal paid home care (Figure 2).
But a care gap is emerging as the baby boom generation ages. The traditional caregiver population (ages 45 to 64) is shrinking while the number of oldest-old Americans—those most likely to need care—is growing. By 2040, there are expected to be just three traditional caregivers per person ages 80 or older—down from a 6:1 ratio in 2025, according to Census Bureau projections.
But there is some good news, Hotz adds. While research finds that adult children feel less obliged to care for stepparents, new evidence suggests that an increasing share of adult children are stepping up when older parents are in need (for example, having trouble buying food). His own analysis shows that childless older people received as much help from their siblings, other relatives, and friends as their peers received from their adult children.
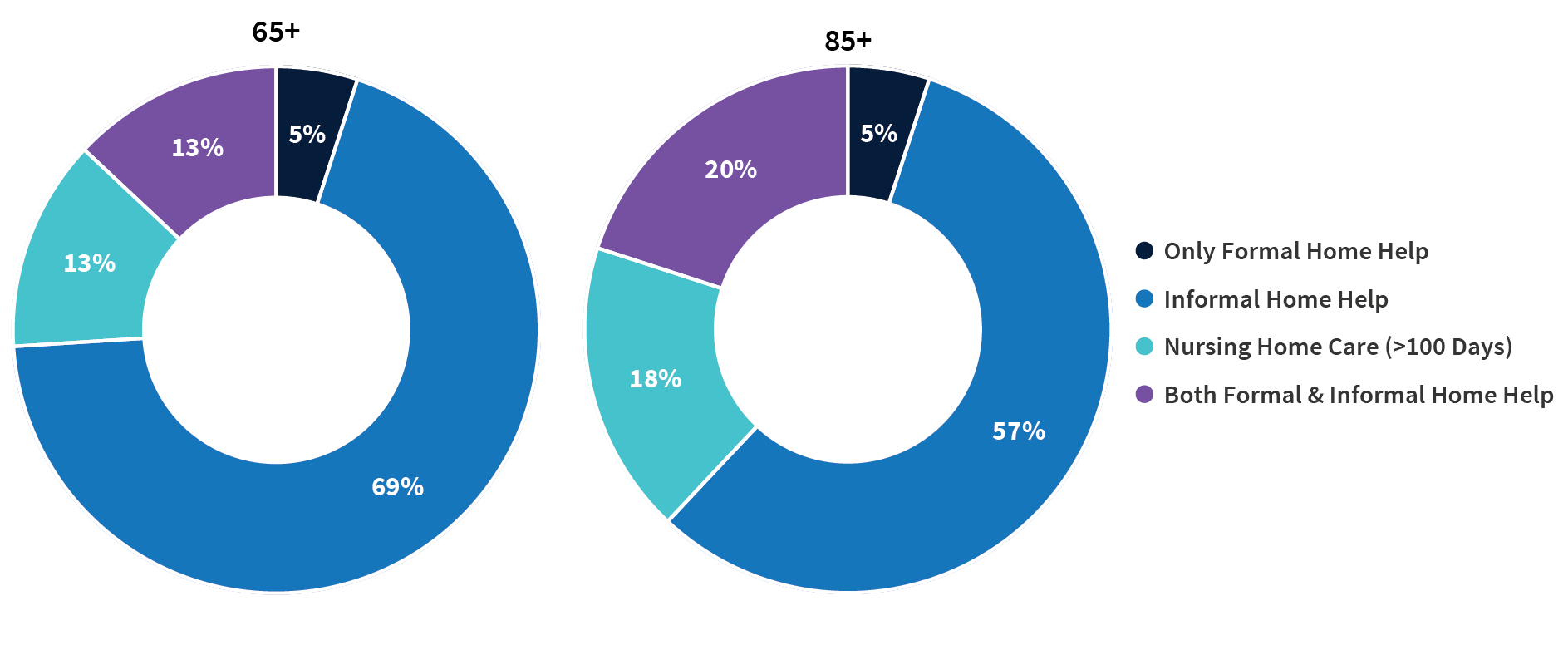
Source: Jonathan Gruber and Kathleen M. McGarry, “Long-term Care in the United States,” National Bureau of Economic Research, Working Paper 31881, November 2023, DOI 10.3386/w31881.
Compared with their peers who have supportive families and robust social networks, socially isolated older people face a greater risk of early death, dementia, heart disease, diabetes, and a host of other conditions, explained Debra Umberson of the Center on Aging and Population Sciences at the University of Texas at Austin. “The evidence is increasingly convincing, overwhelmingly persuasive,” she said.
Inflammation, depression, hypervigilance, alcohol consumption, and the disadvantages of lower levels of education all play a role in poorer outcomes among older adults, Umberson said. Social isolation is a modifiable risk factor; the challenge is “identifying who is most at risk, why, and what can be done.”
Research suggests that “isolation begins to increase as early as adolescence and continues steadily through the life course,” she reported. Black Americans, people living in poverty, and sexual and gender minority populations tend to experience higher levels of isolation than other groups. Experiencing the death of a family member, extreme weather events (like Hurricane Katrina, which dispersed community members), pandemics (as we saw with COVID-19), incarceration, and deportation can also disrupt families and communities.
In 2024, more than half of Americans ages 65 and older (54%) were enrolled in the Medicare Advantage program, up from just 19% in 2007. The dramatic change from a fee-for-service model to a privately run managed care model has vast implication for aging Americans, said Dan Polsky of the Johns Hopkins’ Economics of Alzheimer’s Disease and Services (HEADS) Center. Medicare Advantage plans may offer efficiency and flexibility that can lower recipients’ costs and increase access to home-based care, which most Americans say they prefer, according to Polsky. But new findings by Lauren Nicholas suggest that unpaid family caregivers may be providing more end-of-life home care for people with dementia, essentially moving costs from the formal system of payment to unpaid family members, he reported.
At the same time, traditional Medicare is not without innovations: A new program is exploring ways to meet the health care needs of both people with dementia and their caregivers, Polsky noted.
In the pipeline are new disease-modifying pharmaceutical treatments for dementia, but they require an early diagnosis, which only a fraction of people receive. Should these treatments scale, it could cost the Medicare program tens of billion dollars a year, presenting an additional challenge to the already-strained Medicare budget. Implementing new early diagnosis techniques and providing cost-effective new treatments will present complicated hurdles for the health-care delivery system, Polsky suggested.
The more than 5 million family members and friends who provide unpaid care for older adults with dementia have high—and increasing—demands on their time, reported Jennifer Wolff of the HEADS Center, based on her team’s research using nationally representative data.
On average, the time that family caregivers spent helping older adults with dementia grew by almost 50% between 2011 and 2022, going from 21 hours per week to 31 hours (Figure 3). By contrast, time spent assisting older adults without dementia fell during the same period.
Wolff and team show that more than half (52%) of dementia caregivers lived with the person they were caring for in 2022, up from 39% in 2011. And the share able to hold jobs—outside their caregiving work—dropped from 43% to 35% during the same period.
Noting that the number of individuals affected by dementia is projected to triple in the next 30 years, Wolff underscored the importance of monitoring unpaid caregivers and developing interventions to support them. Some strategies could include providing direct financial assistance and tax relief, supporting flexible work arrangements and paid family leave, and using digital tools and remote monitoring technologies to help caregivers manage care more efficiently and connect with support networks.
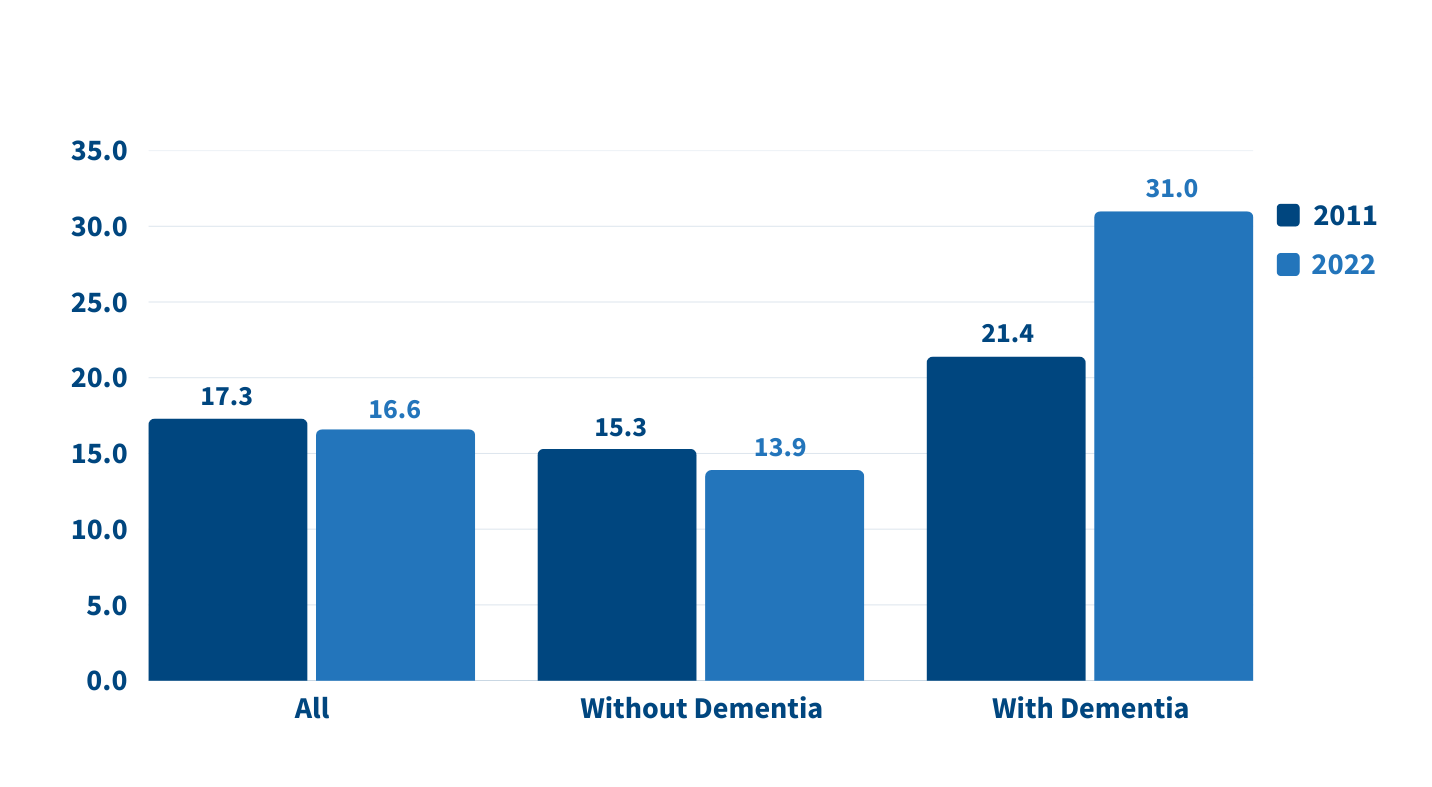
Source: Jennifer L. Wolff, Jennifer C. Cornman, and Vicki A. Freedman, “The Number of Family Caregivers Helping Older US Adults Increased From 18 Million to 24 Million, 2011–22,” Health Affairs 44, no. 2 (2025): 189-95.
More devastating fires, storms, and hurricanes, along with greater climate variability are the “new normal,” said Elizabeth Frankenberg of the Carolina Population Center at the University of North Carolina at Chapel Hill.
People who experience these events not only face an increased risk of death and disease but also lost livelihoods, diminished assets, and poor quality of life for months, years, and even decades to come, she noted.
Older people can be uniquely vulnerable due to reduced physical mobility, cognitive decline, diminished temperature regulation, and changes in economic resources, access to safety net programs, and the availability of social and family networks. Further, their ability to cope with change may be influenced by anxiety around uncertainty, a deep attachment to where they live, and difficulty making life-changing decisions.
To effectively plan for, mitigate, and adapt to severe weather events and temperature changes, demographers should team up with engineers to better understand the level of vulnerability in specific risky locations, Frankenberg said. For example, older people with lower incomes and limited mobility may need emergency support in places with rising sea levels or that are prone to wildfires.
The experts noted several promising areas for future research that can improve the health and well-being of older adults, including:
The researchers emphasized that many of these priorities require sustained investment in longitudinal data collection and interdisciplinary collaboration across aging research centers.
The scholars featured above lead many of the 15 research centers on the demography and economics of aging and Alzheimer’s disease and Alzheimer’s related dementias supported by the National Institute on Aging (NIA) of the National Institutes of Health for the past 30 years.
A coordinating center based at the University of Michigan supports the dissemination of findings from the centers in partnership with PRB.


Senior Research Associate

Research Analyst
Senior Vice President, Programs
New data released by the Appalachian Regional Commission (ARC) and PRB in the 15th annual update of The Appalachian Region: A Data Overview from the 2019-2023 American Community Survey shows that rates of labor force participation and homeownership continue to improve in Appalachia.
Drawing from the latest American Community Survey and comparable 2023 Census Population Estimates, the report, known as “The Chartbook,” contains more than 300,000 data points comparing Appalachia’s regional, subregional and state data with the rest of the nation.
Key improvements in the region’s economic indicators are as follows:
Decrease in unemployment rates and higher labor force participation
Homeownership bypasses national average
Below average number of cost burdened households
“While Appalachia continues to make progress toward reaching economic parity with the rest of the country, it’s important to recognize there is still work to be done,” said ARC Federal Co-Chair Gayle Manchin. “ARC will continue to partner on the local, state, and federal levels to prioritize the future of Appalachia’s 13 states and remains committed to ensuring Appalachians have access to the education, job training and infrastructure they need for prosperous lives in the places they love.”
“This year’s Chartbook highlights important economic advances, not only in Maryland but across the Appalachian Region—including gains in employment and homeownership,” said ARC 2025 States’ Co-Chair, Maryland Governor Wes Moore. “By working together, we continue to uplift our most vulnerable populations, promoting a better, brighter future for all families across Appalachia.”
Despite positive trends, several data points revealed key challenges affecting Appalachian economies compared to the rest of the nation:
Despite population increase, growth lags
Post-secondary educational attainment remains behind national average
Greater share of Appalachians live in poverty
“The data point to bright spots but also guide us to areas where targeted efforts could improve well-being for Appalachians across the region,” said Sara Srygley, a senior research associate at PRB. “Decisionmakers and advocates can use the Chartbook to create the changes they want to see in their communities.”
The data shows that Appalachia’s rural areas continue to be at increased risk for economic distress compared to its urban areas. Appalachia’s 107 rural counties are also more uniquely challenged, compared to 841 similarly designated rural counties across the rest of the U.S., as rural Appalachian counties continue to lag behind on indicators including educational attainment and household income.
The data also highlights key differences between Appalachia’s subregions, including:
In addition to the written report co-authored by the Population Reference Bureau, ARC offers companion web pages on Appalachia’s population, employment, education, income and poverty, computer and broadband access, and rural Appalachian counties compared to the rest of rural America’s counties. For more information, visit www.arc.gov/chartbook.
About the Appalachian Regional Commission
The Appalachian Regional Commission is an economic development entity of the federal government and 13 state governments focusing on 423 counties across the Appalachian Region. ARC’s mission is to innovate, partner, and invest to build community capacity and strengthen economic growth in Appalachia to help the region achieve socioeconomic parity with the nation.

Associate Vice President, U.S. Programs
Contributing Senior Writer
As the large Baby Boom generation enters advanced ages, more family members and other unpaid helpers are stepping in as caregivers. In just over a decade, the number of family caregivers regularly assisting older adults with daily activities at home grew by 32%, increasing from 18.2 million to 24.1 million between 2011 and 2022.1
While the caregiving cadre has grown, who’s getting care has also changed. Older Americans receiving family care are younger, better educated, and less likely to have dementia than they were in 2011, report Jennifer L. Wolff of Johns Hopkins University, independent consultant Jennifer C. Cornman, and Vicki A. Freedman of the University of Michigan.
The increase in family caregiving partly reflects the rising share of older adults with multiple chronic conditions, such as heart disease, hypertension, stroke, and cancer. And while the share of older adults with dementia has declined, unpaid caregivers average twice as many hours each week caring for people with dementia than without dementia (about 31 hours versus 14), Wolff and team found (see Figure 1).
In addition, a new study estimates that the number of new dementia cases will double over the next 40 years as the population ages—setting the stage for more demands on dementia caregivers and more changes to the caregiving landscape.
“Understanding the changing composition and experiences of family caregiving has never been more important, but it is challenging to assess,” the researchers write. “[It] requires consistent measurement for well-characterized, generalizable samples of people who receive and provide help.”
The nationally representative National Study of Caregiving and the National Health and Aging Trends Study offer important insights. The two studies provide a snapshot of the family caregivers that help Americans ages 65+ who live in the community (i.e., at home or with a relative) or in a residential care setting other than a skilled nursing facility, such as an assisted or independent living facility, a personal care home, or a continuing care retirement community.
Family caregivers include relatives and unpaid helpers, like neighbors and friends, who assist with personal care tasks like bathing and dressing; mobility tasks like getting out of bed and getting around the house; and household activities such as laundry, food preparation, shopping, and managing money.
On average, the time that family caregivers spent helping older adults with dementia increased by almost 50% over the decade, rising from 21.4 hours per week in 2011 to 31.0 hours in 2022. By contrast, time spent assisting older adults without dementia fell from 15.3 hours a week in 2011 to 13.9 hours in 2022 (Figure 1).
Source: Jennifer L. Wolff, Jennifer C. Cornman, and Vicki A. Freedman, “The Number of Family Caregivers Helping Older US Adults Increased From 18 Million to 24 Million, 2011–22,” Health Affairs 44, no. 2 (2025): 189-95.
People caring for older adults with dementia have high—and increasing—demands on their time. More than half (51.7%) of dementia caregivers lived with the person they were caring for in 2022, up from 39.4% in 2011, Wolff and team report. And the share able to hold jobs—outside their caregiving work—dropped from 42.5% to 34.6% during the same period.
Among caregivers with formal jobs, the share who reported challenges with their employment—including working fewer hours or being less productive—increased over the decade, regardless of whether they cared for someone for dementia.
“Challenges are exacerbated when caregivers are in poor health themselves; have a lack of choice in assuming the caregiving role; and, for the substantial proportion of family caregivers who are employed, work in low-wage jobs with limited flexibility,” the researchers note.
Which older Americans get family care? As in the past, they tend to be female, non-Hispanic white women who are married or widowed. But growing numbers of family care recipients are male and have some college education. More are also separated and divorced compared to 2011, reflecting national trends.
Who’s providing care? Family caregivers continue to be largely female and married, and most report being in good health. In 2022, adult children still made up the largest share of family caregivers for older adults, at 40.7%, but this represents a significant decline since 2011 (Figure 2).
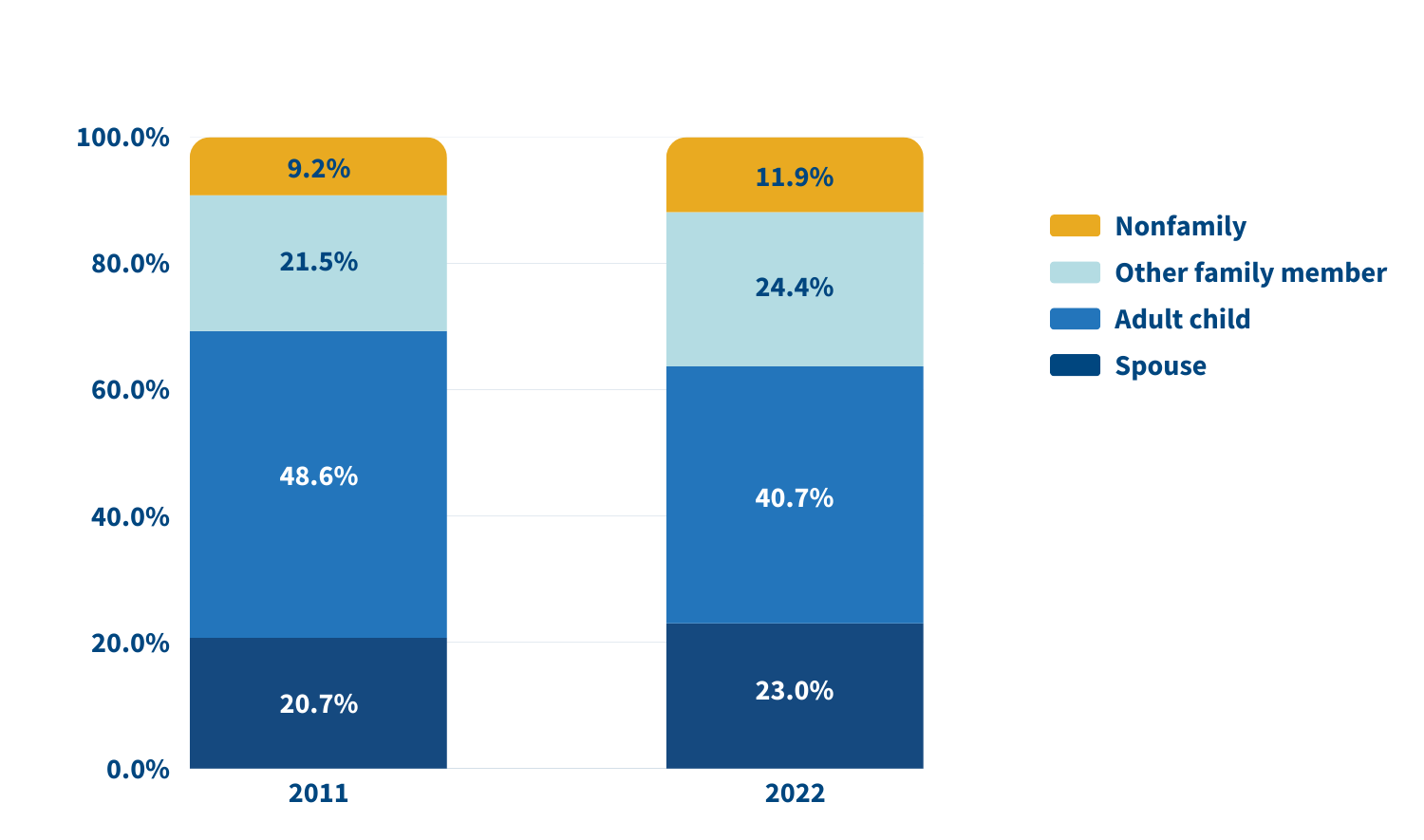
Source: Jennifer L. Wolff, Jennifer C. Cornman, and Vicki A. Freedman, “The Number of Family Caregivers Helping Older US Adults Increased From 18 Million to 24 Million, 2011–22,” Health Affairs 44, no. 2 (2025): 189-95.
In 2022, adult children accounted for about half (49.1%) of family caregivers for older adults with dementia, compared with 38.4% of caregivers for those without dementia. Just 17.7% of family caregivers for older adults with dementia were spouses, compared with 24.5% of family caregivers for people without dementia.
A sizeable share of family caregivers (17.0%) had children under age 18 at home in 2022, and 6% to 13% viewed their care responsibilities for older adults as a source of financial, physical, or emotional difficulty.
Despite these challenges, the researchers report a decline in the use of support groups (4.1% to 2.5%) and respite services (12.9% to 9.3%) between 2011 and 2022.
Many caregivers face extraordinary demands and should be the focus of support services, Wolff and colleagues say. They single out those caring for older adults with dementia or nearing the end of life, as well as caregivers “from racial and ethnic minority groups who are more likely to assist people who have extensive care needs in circumstances that involve scare economic resources.”
Family care needs are likely to rise as the number of U.S. adults ages 85 and older is projected to triple by 2050. The researchers note that the number of family caregivers rose even as the long-term use of skilled nursing facilities among older Americans dropped and community living increased. The challenges these caregivers continue to face is “sobering,” they write, including competing time demands from work and child care while spending an average of 17 hours per week on care. In addition, about 1 in 8 family caregivers report financial, physical, or emotional difficulties related to their caregiving roles, percentages that were largely unchanged over the 11 years examined.
Policies and programs to help reduce the financial, physical, and emotional burden of caregiving exist, but do not represent a coherent strategy, the researchers say. “Local, state, and federal policies are a patchwork that is uneven in availability and largely symbolic in magnitude,” they argue. Addressing the needs of family caregivers will require a “cohesive framework in support of the care economy.”
1. Jennifer L. Wolff, Jennifer C. Cornman, and Vicki A. Freedman, “The Number of Family Caregivers Helping Older US Adults Increased From 18 Million to 24 Million, 2011–22,” Health Affairs 44, no. 2 (2025): 189-95.
Exploring New Ways to Use Data for Good
Since Population Reference Bureau’s (PRB’s) founding in 1929, the world has changed tremendously and PRB has evolved along with it. We continue to explore new ways of working (globally, locally, even remotely) and hone our expertise to offer solutions relevant to today’s health and well-being challenges, such as the growing prevalence of noncommunicable diseases and the increase in anxiety among young people. What hasn’t changed is PRB’s impact on informing evidence-based practices, which you’ll see highlighted in this report.
In Fiscal Year 2023, we reached wide audiences with analyses and assessments on issues such as population aging, climate adaptation, maternal health, unpaid care work, and big data. We partnered with organizations like the Conrad N. Hilton Foundation, Regional Consortium for Research on Generational Economy, Southern California Association of Governments, and William and Flora Hewlett Foundation. And the people who work here have made it all possible.
Part of any organization’s evolution is change in those people. From PRB’s original staff of 8 to 55 today, we’ve seen a lot of great people walk through our doors. In late 2022, we welcomed a new Vice President to lead our U.S. Programs, Diana Elliott. Midway through 2023, we appointed our first Africa Director, Aïssata Fall. And just a few months ago, PRB’s Board of Trustees appointed me as President and CEO. PRB’s new leadership is guided by the organization’s strategic plan to explore new areas of focus and ways of working while keeping population and demographic data at the core of what we do. It is a strong foundation from which to move forward toward our 100th year in 2029.
Our partners outside the organization are also essential to PRB’s success. My predecessor, Jeffrey Jordan, collaborated with other international organizations in 2023 on the TIME Initiative, an ongoing effort to answer hard questions about the evolving role of international nongovernmental organizations working in sexual and reproductive health and rights. I am pleased to be stepping into this space as I take the helm at PRB.
Barbara Seligman, Senior Vice President of International Programs, led the way in making PRB’s presence more prominent in 2023 as she advocated for our return to hosting more public events like the webinar on young Africa’s potential to power the global workforce. Diana Elliott quickly became another energetic force behind PRB’s increased public engagement, from authoring blogs that delve into the heart of current population concerns to speaking with the media and other organizations. And Reena Atuma, our Team Lead in Kenya, works daily alongside staff and local officials, youth, and others on concrete policy changes aimed at improving people’s health.
There’s so much more. We’ve captured some of the highlights for you in this year’s annual report.
Sincerely,
![]()
President and CEO

![]()
Under the PROPEL Health project, we worked with partner radio stations and community youth in nine districts across Malawi to raise awareness of social challenges around topics concerning nutrition, education, and health services; and harmful cultural norms like child marriage. We supported these local actors in their efforts to make context-specific, change-oriented information on these topics available in their communities and get people talking about them.
And they’ve made an impact.
Local radio programs in Malawi are now using their platform to hold leaders accountable for enforcing the child marriage law, and they are educating communities on how to respond to and prevent gender-based violence.
After a series of radio programs on child, early, and forced marriage and gender-based violence aired, a traditional authority in Monkey Bay in Malawi’s Southern Region publicly committed to enforcing the law against child and forced marriage, stating, “Dzimwe Radio has been insisting that I intervene and show my commitment in dealing with child marriages—hence my order to demote those village heads [found to not be enforcing the law].” In Mchinji, in Malawi’s Central Region, local police began holding town meetings about gender-based violence, and community members involved police and victim support units in investigations that led to the dissolution of child marriages, and arrests and fines for adult perpetrators.
And after Mudzi Wathu Radio aired programs about youth mental health challenges and the lack of available care, Mr. Biziwiki Mwatibu Banda, the clinical officer at Mchinji District Referral Hospital, announced, “We are very thankful to Mudzi Wathu Community Radio for giving youth a platform to express their views and present their complaints… After hearing those complaints, our management decided to train one health care provider from each of the 21 health centers, aiming to provide mental health counseling in all rural areas.”

In the process of spurring these positive changes—and many more like them—the young people involved in this work learned valuable skills that help provide them with more academic and professional opportunities.
Black women in the United States face a high risk of death from pregnancy-related complications. Most of these deaths are preventable, according to a study by the Centers for Disease Control and Prevention. “We need new models of care before, during, and after birth to address these inequities,” says Marie Thoma, a reproductive and perinatal epidemiologist and population health scientist at the University of Maryland.
To raise awareness of the Black maternal health crisis in the United States, PRB partnered with creative agency TANK Worldwide and Dr. Shalon’s Maternal Action Project on a 2023 national campaign. It featured data from PRB’s article on NICHD-funded research that found U.S. Black women are 3.5 times more likely to die of pregnancy and postpartum complications than white women. With our partners, we promoted the campaign and research through social media, a press release, and fact sheet, and caught the attention of media, including NPR’s Here and Now. The campaign won a Clio Health award, which recognizes creative marketing and communications in the fields of physical, mental, and social well-being.
Read our follow-up interview with Marie Thoma about emerging research on this crisis.
How can local learning drive global solutions? This question is one we ask daily on the MOMENTUM Knowledge Accelerator project, which is part of USAID’s larger MOMENTUM program that seeks to improve the health and well-being of women, children, and families in more than 38 countries. Part of the project’s role is to identify and share best practices that can be applied across the different settings where MOMENTUM works.
In 2023, MOMENTUM Knowledge Accelerator brought together project staff who are working with their country counterparts to adopt and adapt the World Health Organization’s model of care for small and/or sick newborns in Indonesia, Mali, Nepal, and Nigeria. The goal? Develop a set of common questions and tools to learn about the model’s early rollout in different settings. For instance, how acceptable is the model in these settings? How feasible is it to implement the model in the different country contexts and settings? What adaptations are needed to the model based on the health systems’ contexts? The experiences in each country so far show that when health system and community actors are properly engaged, the model is acceptable, appropriate, and feasible in each setting. If governments can continue to provide resources to support the model’s different elements, more newborns can survive and thrive.
Using this information, we are working to share common approaches and address factors like how different aspects of the health system and variations between the public and private sectors affect the model’s implementation. Identifying and sharing such early insights can help shape global learning and strengthen the quality of care that small and sick newborns receive from their local health care providers—changing and improving lives.
This example is just one of the ways that we collaborate and communicate, gathering and assessing knowledge to share insights that people can put into practice.

Resources—and financial burdens—flow from one generation to another. Understanding how it happens is key for governments focused on fostering sustainable development, and data from national transfer accounts (NTA) can provide key insights.
In 2023, PRB and the Regional Consortium for Research on Generational Economy (CREG) hosted a shared space in Senegal to make complicated topics like the value of women’s unpaid labor easy to understand so decisionmakers could assess needs and accountability. The 3rd National Transfer Account–Africa Conference in La Somone-Senegal, held in partnership with CREG, PRB, the United Nations Population Fund, and United Nations Economic Commission for Africa, brought together more than 130 participants from 19 African countries, including parliamentarians and decisionmakers from various ministries.

The Africa NTA Network, drawn by our reputation for facilitating high-level policy dialogue informed by data, chose PRB to moderate three of four plenary conference sessions. Africa Director Aïssata Fall facilitated a session on the importance of unpaid care work and achieving a demographic dividend, which featured key messages developed by PRB policy communication fellows participating in the conference. She also directed two plenary sessions focused on high-level policy dialogue with parliamentarians and decisionmakers from ministries of planning, budget, gender, and social affairs. They came together to discuss challenges related to the demographic dividend and the care economy and the difficulty of translating these complex and often-abstract concepts so they can be considered in practical applications.
We developed a three-part climate blog series in English and French to advance a new approach to investments in climate adaptation that integrate population, gender, health, and the environment. The series lays the foundation of a people-centered framework for building resilience to climate change centered on agency, equity, and the power of local solutions.
And, in a year that closed as the hottest on record, solutions are more urgent than ever, as is knowing how—and which—populations will be most affected by climate change. Population characteristics like age, gender, and socioeconomic status are a few of the factors that make some people more vulnerable to the effects of a changing climate. Understanding them can help countries adapt and build resilience to future climate-related events, and we put a spotlight on this topic in our 2023 World Population Data Sheet.
We also worked with researchers participating in the 2023 ARUA Climate Change and Inequalities Symposium at the University of Cape Town to provide feedback and coaching on their presentations, which were focused on social inequalities and climate change action, so they could deliver clear, compelling messages. Read our top five tips to make your presentation message stand out.
The year 2023 marked the official end of the COVID-19 state of emergency. Yet the disease continued to spread, and many people continued to feel its effects. Decisionmakers need evidence of these impacts so they can effectively plan for their communities.
PRB’s KidsData program released data and findings from the Family Experiences During the COVID-19 Pandemic survey that highlighted ongoing challenges. The survey checked in with parents and caregivers four times to track the pandemic’s evolving impact on families. The results released in 2023 showed persistent challenges for California families despite suggestions that life had returned to normal.

In California, three years after the pandemic’s onset, children still faced significant COVID-related challenges, and their caregivers remained concerned. As safety-net supports began to roll back, nearly half of parents and caregivers statewide (45%) said their household finances were negatively impacted since the start of the pandemic, up from 32% a year prior. And more than half (58%) said they worried for the safety of their children as public health measures, like masking mandates, relaxed. Rates of concern were even higher in households with children with special health care needs.
The pandemic’s effects on young people are of particular concern as adverse childhood experiences, especially in early childhood, can have negative, long-term impacts on health and well-being. KidsData remains committed to tracking and analyzing data on the health and well-being of California’s children.
How can gender-transformative approaches and programming help improve outcomes for family planning and reproductive health? How can we address the gender inequities that global health workers experience? What are the links between sexual and reproductive health and technology-facilitated gender-based violence? What intersectional approaches are being applied to gender-transformative programming? How can comprehensive sexuality education help strengthen gender-based violence prevention and response efforts and vice versa?
If you are among the more than 2,600 members of the Interagency Gender Working Group (IGWG), you may already know the answers to these questions.
For 13 years, PRB managed the IGWG, a community of practice founded nearly 30 years ago to promote gender-sensitive considerations as a critical factor in improving family planning and reproductive health outcomes and advancing sustainable development.
Under our management, the IGWG highlighted best practices, challenges, and opportunities for promoting gender equality through global health programming, showcased the work of gender experts and advocates around the world, and led discussions on cutting-edge topics on and approaches to gender-transformative health programming.

In late 2023, we transitioned management of the IGWG to the PROPEL Youth and Gender project. During its time with PRB, the IGWG served as a reputable resource for gender experts, advocates, and program implementers working in global health and other sectors. It centered and elevated the voices of gender experts, advocates, and researchers, with special attention to locally led efforts, and the community of practice made notable contributions to the field with products that captured a wealth of knowledge and actionable recommendations for practitioners, advocates, researchers, and donors.
Both seasoned experts and those just beginning to integrate a gender-sensitive lens into their activities rely on materials like the IGWG’s newsletter and signature Gender Integration Continuum, a valuable tool for program implementers that measures whether and how interventions incorporate gender equity to improve development outcomes.
Explore some of our work with the IGWG:
We look forward to watching the IGWG’s continued growth and success.
As part of our activities on the Stawisha Pwani project, we collaborated with county officials, youth, and others in four coastal counties in Kenya as they sought to create and strengthen policies concerning the health of people in their communities.
We worked with officials in Mombasa County’s Department of Health to bring together youth representatives, county officials, and other stakeholders in the private sector and at nongovernmental organizations to develop the Mombasa County Adolescent and Young People Strategy on Health for 2024-2029. In our role of helping to facilitate dialogue, we drafted a template for the strategy and a plan for communicating its benefits to decisionmakers, and then formed a youth technical working group to draft, review, and revise the policy before it was shared with stakeholder groups for their feedback.

This collaborative process resulted in a strategy—approved by the Mombasa County government—that is in use today, helping to guide decisions across County departments on high impact programming for adolescents and young people.
In Taita Taveta County, we helped advance policy change by providing technical assistance to officials reviewing the Health Financing Facility Improvement Fund (FIF) law and developing the FIF operations and supervision manual. The FIF provides a way to collect and manage revenue from the health services delivered by public health facilities, as well as for these facilities to use the revenue to improve service delivery. The County and Subcounty Health Management Teams are relying on the manual as they monitor revenue collection to ensure resources are being used practically and to increase accountability.
The manual’s guidelines and revisions to the FIF law that allow facilities to retain and use revenue—a key element for strengthening health systems in Taita Taveta—contributed to the Department of Health surpassing its FIF collection targets for Fiscal Year 2022-2023. The Taita Taveta County Annual Development Plan 2024/25 reports that the collection goal of KES 100,000,000 was exceeded by more than 50%, for a total of KES 161,118,235. The health facilities can use these additional resources to further improve their efforts to meet the needs of the communities they serve.
![]()
PRB produced articles, blogs, reports, webinars, and other materials in 2023 on a range of topics such as climate adaptation, gender equality, population aging, unpaid care work, and the U.S. labor shortage. Explore some of these works here.
2023 World Population Data Sheet
A New Approach for Climate Resilience
Elements of Climate Resilience: The Foundations of a People-Centered Framework
Five Actions to Help Build Equitable Climate Resilience
Gender Equity for Work and Pay
Eight Demographic Trends We’re Watching as the World Population Passes 8 Billion
PRB CEO Calls for Restoring Public Trust in Data at United Nations Development Event
Comment l’autosoin peut soutenir la résilience en Afrique de l’Ouest et du Centre
How Self-Care Can Support Resilience in West and Central Africa
To Fix the Care Economy, the United States Should Look Internationally
Want Another Perspective on the U.S. Labor Shortage? Talk to a Demographer
The generous support we receive from organizations and individuals helps make our work possible. Thank you.
PRB worked together with 19 organizations in 2023.
Through their generous contributions, the individuals listed here allowed PRB to fund essential program expansion and organizational innovations during the fiscal year ending Sept. 30, 2023.

Senior Research Associate
New data released today by PRB and the Appalachian Regional Commission shows that rates of labor force participation, educational attainment, income, and poverty continue to improve in Appalachia.
The 14th annual update of The Appalachian Region: A Data Overview from the 2018-2022 American Community Survey draws from the latest American Community Survey and comparable 2022 Census Population Estimates. Known as “The Chartbook,” the report contains more than 300,000 data points comparing Appalachia’s regional, subregional, state, and county economic status with the rest of the nation.
Key improvements in the region’s economic indicators are as follows.
Increased income and lower poverty rates
Higher educational attainment and labor force participation
Increased population growth in south
Increase in broadband access
“We celebrate the progress Appalachia has made, including declined poverty rates and increased broadband access. However, we know that there is still much work to be done for our entire region to reach economic parity with the rest of the country,” said ARC Federal Co-Chair Gayle Manchin. “ARC will continue to prioritize the quality of life of Appalachia’s 26 million residents, and remains committed to continued collaboration across federal, state, and local levels to ensure our people have a bright future.”
Despite positive trends, several data points revealed vulnerabilities that emphasize the inequities in Appalachia compared to the rest of the nation:
Overall population decline
Poverty rates for children and families and specific counties
Disability and poverty in older adults
Despite gains in access, digital divides persist
“The data in this year’s Chartbook highlight strides being made in the Appalachian Region, with noteworthy improvements across economic, educational, and health-related measures,” said Sara Srygley, a senior research analyst at PRB. “Yet, these data also emphasize considerable variation throughout the region—particularly the persistent challenges facing rural communities.”
The data show that Appalachia’s rural areas continue to be more vulnerable than its urban areas. Appalachia’s 107 rural counties are also more uniquely challenged, compared to 841 similarly designated rural counties across the rest of the U.S. Though rural Appalachians did have higher health insurance coverage than the rest of rural America, rural Appalachian counties continue to lag behind on educational attainment, labor force participation, broadband access, household income and population growth.
The Appalachian Region: A Data Overview from the 2018-2022 American Community Survey was written by PRB and the Appalachian Regional Commission.
In addition to the written report, ARC offers companion web pages on Appalachia’s population, employment, education, income and poverty, computer and broadband access, and rural Appalachian counties compared to the rest of rural America’s counties. For more information, visit www.arc.gov/chartbook.
The Appalachian Regional Commission is an economic development entity of the federal government and 13 state governments focusing on 423 counties across the Appalachian Region. ARC’s mission is to innovate, partner, and invest to build community capacity and strengthen economic growth in Appalachia to help the region achieve socioeconomic parity with the nation.