Mark Mather
Associate Vice President, U.S. Programs

Dementia is one of the nation’s most expensive old-age health conditions and the most time consuming for family caregivers. As many as 6 million people ages 65 and older live with Alzheimer’s disease in the United States, representing about one in 10 older Americans.1
However, rates of dementia are not uniform across the older population. Those with lower levels of education, the oldest old (people ages 85 and older), women, and racial and ethnic minorities are at greater risk of dementia. The types of living arrangements of people with dementia—whether they live at home, in a residential care setting (such as assisted living), or a nursing facility—also differ depending on the availability of family caregivers and financial resources.
This issue of PRB’s Today’s Research on Aging (Issue 40) summarizes what we know about the characteristics of people with dementia and their caregiving and living arrangements based on studies funded by the National Institute on Aging. Understanding the characteristics of those with dementia can help lawmakers design policies that better meet the needs of this rapidly growing population and their families.
Many conditions and diseases can cause dementia—a set of symptoms that may include memory loss and difficulties with thinking, problem-solving, or language. Alzheimer’s disease is the most common cause, but dementia can also be caused by injuries from impaired blood supply to the brain, often after a stroke. Other types of dementia include Lewy body dementia and frontotemporal disorders.
Alzheimer’s disease and other related dementias are characterized by progressive cognitive decline that interferes with independent functioning. In the National Health and Aging Trends Study (NHATS)—a nationally representative sample of Medicare beneficiaries ages 65 and older—respondents are classified into three categories: those with no dementia, possible (or early stage) dementia, and probable dementia. Participants are classified as having probable dementia if a doctor has told the person that they have dementia or Alzheimer’s disease.
For respondents without a diagnosis, dementia status is determined through a test measuring cognitive functioning, including memory (word recall), orientation (such as knowing the date and year), and executive functioning (drawing a specific time on a clock). In addition, for respondents unable to self-report, proxy respondents (typically a family member) answer the AD8, a series of eight Yes/No questions about the respondent (problems with judgment, reduced interest in hobbies, repeats self, trouble using tools or appliances, forgets correct month/year, trouble handling finances, forgets appointments, daily problems with memory/thinking).2
Cut points (based on standard deviations from the mean) are then used to group study participants into different categories. In the 2011 NHATS, 11% of Medicare beneficiaries ages 65 and older were classified as having probable dementia (10% among the non-nursing home population).3
Clinical guidelines developed by the National Institutes of Health and the Alzheimer’s Association also define three stages of Alzheimer’s disease (the most common type of dementia):
People with advancing dementia (or moderately severe dementia) are more likely to have difficulty with one of three daily living activities (dressing, bathing, or using the toilet) and cognitive difficulties that make it more difficult to manage medications or finances, whereas people with advanced dementia have difficulty with all these functions and more.5
No cure for Alzheimer’s disease currently exists, and no treatments have been proven to prevent its onset or delay its progression, but researchers are studying ways to treat the disease and expand support for people with Alzheimer’s disease and their families.
Prevalence of Probable Dementia Among the U.S. Population Ages 70 and Older, 2015
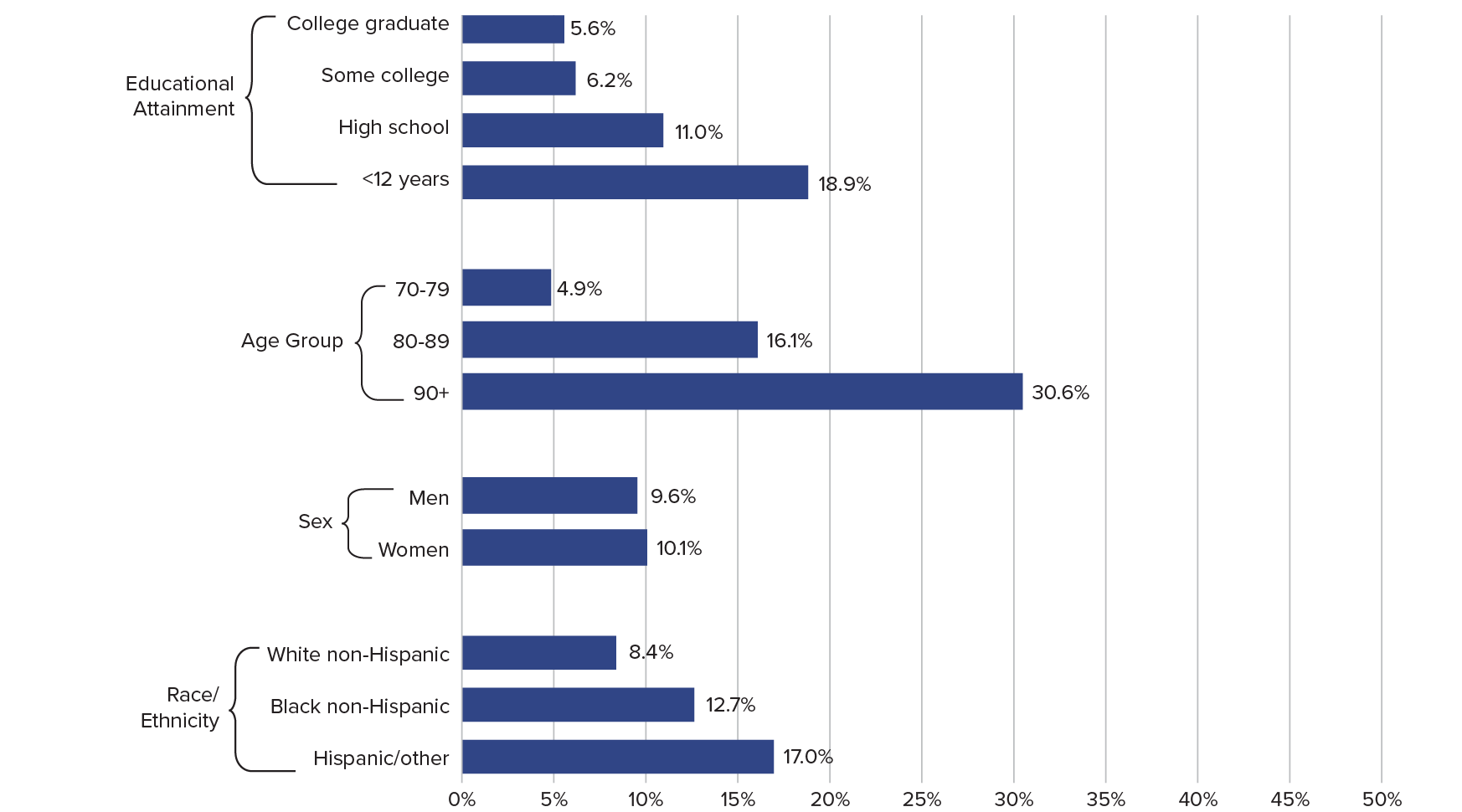
Note: Excludes persons in nursing homes.
Source: Vicki A. Freedman et al., “Short-Term Changes in the Prevalence of Probable Dementia: An Analysis of the 2011–2015 National Health and Aging Trends Study,” Journals of Gerontology, Series B 73 (2018): S48-S56.
Age-Adjusted Death Rates per 100,000 by State, 2017
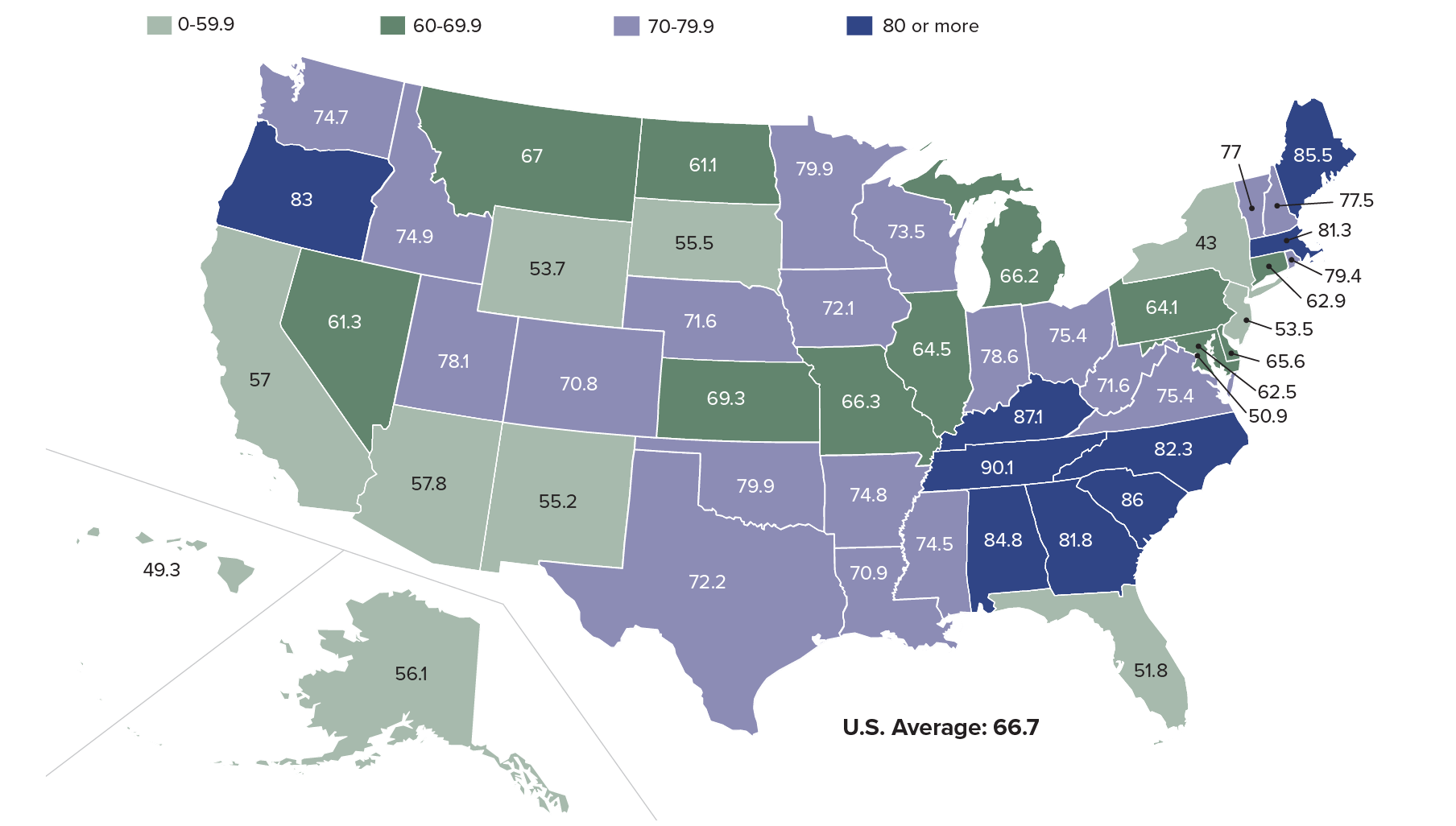
Source: Ellen A. Kramarow and Betzaida Tejada-Vera, “Dementia Mortality in the United States, 2000-2017,” National Vital Statistics Reports 68, no. 2 (2019).
Socioeconomic and Demographic Characteristics of Medicare Enrollees Ages 65 and Older With Advancing Dementia, by Care Setting
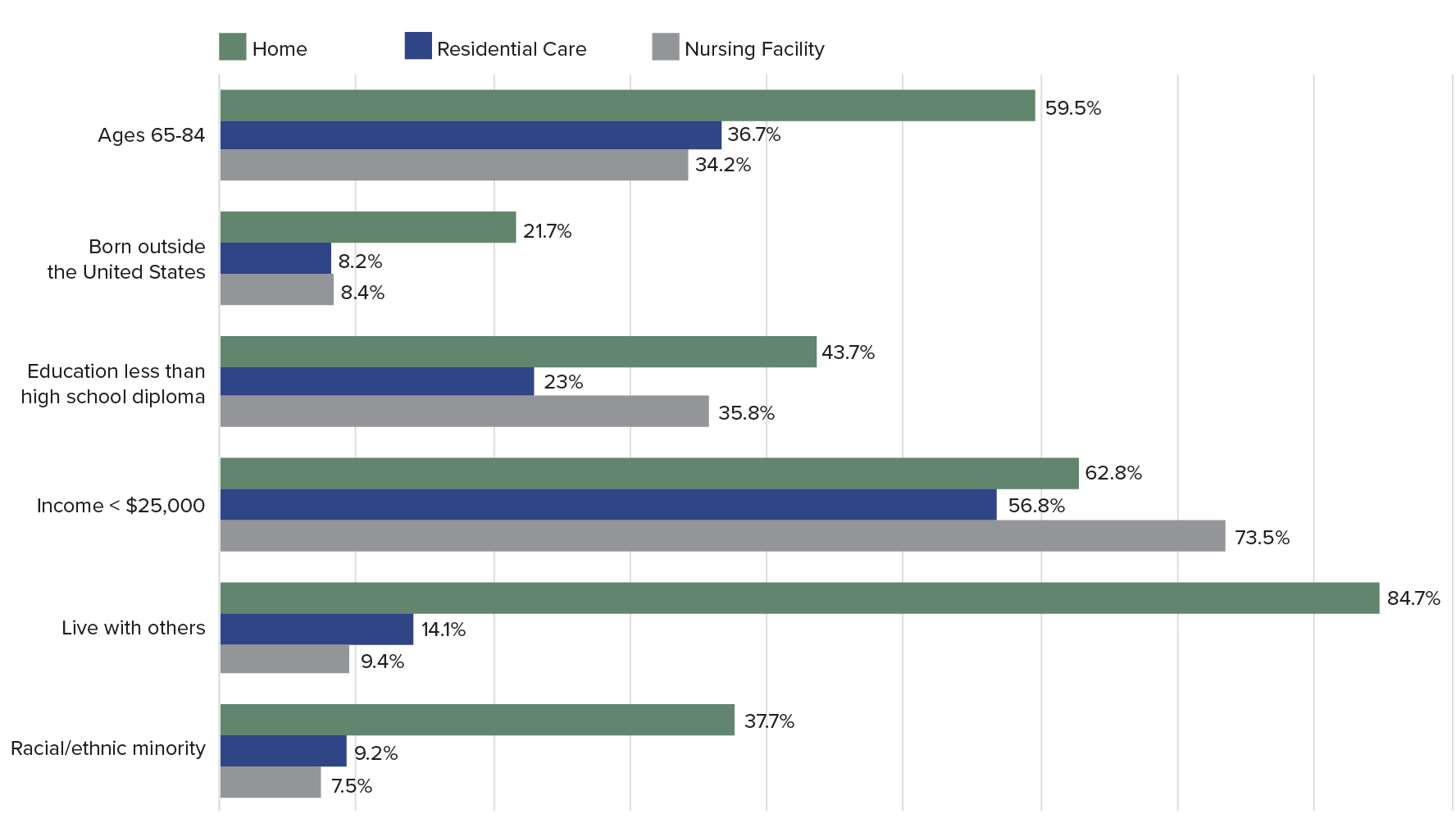
Notes: All differences comparing home versus residential care versus nursing home significant at P > .05. The amount used in many states in 2012 to determine eligibility criteria for Medicaid-paid nursing home care was $25,000.
Source: Krista L. Harrison et al., “Care Settings and Clinical Characteristics of Older Adults With Moderately Severe Dementia,” Journal of the American Geriatric Society 67, no. 9 (2019): 1907-12.
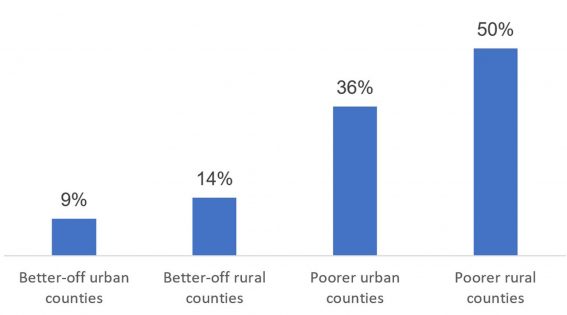
Out-of-Pocket Expenditures on Dementia During the Last Five Years of Life as a Percentage of Wealth, by Population Subgroup
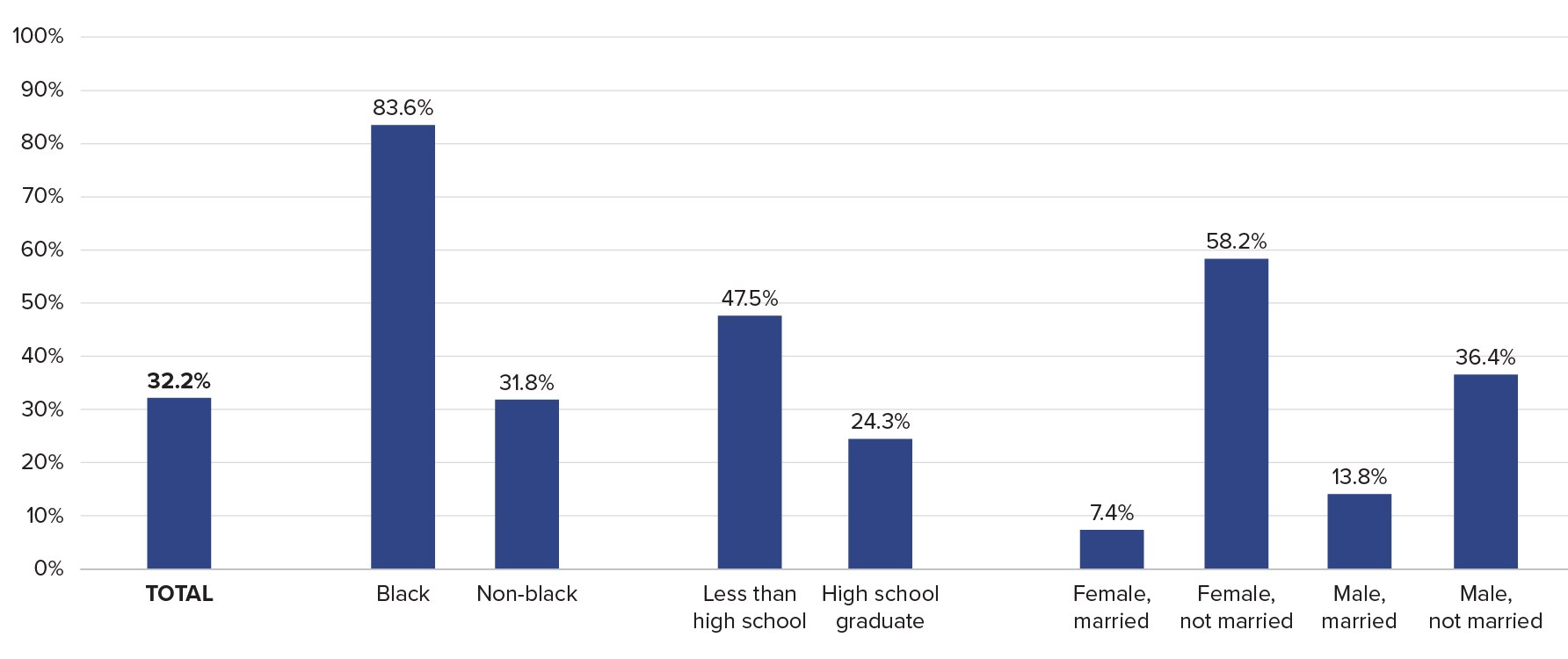
Source: Amy Kelley et al., “The Burden of Health Care Costs for Patients With Dementia in the Last Five Years of Life,” Annals of Internal Medicine 165, no. 3 (2015): 729-36.

No other country in the world is experiencing population aging on the same scale as China.
The United Nations projects that there will be 366 million older Chinese adults by 2050, which is substantially larger than the current total U.S. population (331 million).1By that time, China’s share of adults ages 65 and older wills have risen from just 12% to a projected 26%. This rapid population aging—driven by recent declines in fertility and mortality—raises concerns about the health and well-being of older Chinese adults and will create considerable challenges for the health care system.
While life expectancy in China is increasing, older adults may spend more of their advanced years in poor health and with disabilities. Families have been the primary source of care for older adults, but the country’s rapid economic development and urbanization have separated millions of older adults from their children, contributing to an increasing demand for community-based health care.
These demographic and socioeconomic changes raise important questions for researchers and policymakers. How are older Chinese adults faring relative to their parents’ and grandparents’ generations? How is rapid urbanization affecting health and the availability of potential caregivers among older adults? How are older women faring relative to men, and which factors contribute to the gender gap in health? More broadly, what are the key factors associated with healthy aging in China, and what can policymakers do to improve health and reduce health disparities in the context of the country’s rapid socioeconomic development?
This issue of PRB’s Today’s Research on Aging (Issue 39) summarizes recent research on aging and health in China from U.S. National Institute of Aging-sponsored investigators and surveys, especially the China Health and Retirement Longitudinal Study (CHARLS) and Chinese Longitudinal Healthy Longevity Study (CLHLS). Results from these studies can shed light on the key determinants of healthy aging and help identify policies to address the challenges posed by rapid population aging in China.2The findings can also offer insights to policymakers in other countries with rapidly growing older populations.
China’s life expectancy has increased steadily during the past half century. In 1960, average life expectancy at birth in China was around 44 years. By 2017, it had increased to 76 years.3
Physical and cognitive health among older adults—especially women—is also improving with rising educational attainment and better medical care.4
Yi Zeng and colleagues find evidence of morbidity compression among China’s older adults—a reduction in the proportion of life spent with disability. Among adults ages 80 and older, mortality and self- reported disability rates have fallen relative to cohorts born 10 years earlier, according to their analysis of CLHLS data.5A recent study of adults ages 50 and older, based on CHARLS data, shows that at age 50, men can expect to live 24 years without activity limitations (26 years for women).6
These life expectancy gains and reductions in disability, however, are linked to rapid economic development in urban areas. Older adults in rural areas have not fared as well, leading to growing rural-urban disparities in health.7
Rising obesity rates and high smoking prevalence (among men) also present major health challenges for China’s aging population. In 2011, 28% of men and 38% of women ages 45 and older were overweight, putting them at higher risk of heart disorders, hypertension, diabetes, and stroke.8 Over half of men ages 45 and older (53%) smoked in 2011, compared with 5% of women in that age group.9 High levels of pollution—especially in urban areas—pose additional health risks.
“Public health campaigns and incentives are urgently needed on all these fronts so that the predictable long-term consequences of these behaviors on older age disease are not realized,” report researchers James Smith and his colleagues.9
Source: James P. Smith, Meng Tian, and Yaohui Zhao, “Community Effects on Elderly Health: Evidence from CHARLS National Baseline,” Journal of the Economics of Ageing 1-2 (2013): 50-59.

Sleep may be as important to health in old age as diet and exercise. Numerous studies have shown that sleeping too much or too little is associated with mortality among older adults.
A growing body of research indicates that not getting enough sleep may also increase the risk of several conditions and chronic diseases including diabetes, cardiovascular disease, obesity, and depression.
This issue of PRB’s Today’s Research on Aging (Issue 38) explores National Institute on Aging-supported research on sleep and aging, reviewing new evidence indicating that poor sleep may be both a sign of ill health and a trigger for processes related to disease and biological aging.
While sleep often tends to become more challenging for older people, insomnia—trouble falling asleep and staying asleep—is not a given with old age. The research examined here underscores the importance of screening for poor sleep and interventions that improve the sleep of older people.
Investigators are looking more deeply into the role of sleep in chronic disease and the aging process. Most studies on the relationship between sleep duration and health have been based on self-reported time spent asleep. These studies provide evidence of a U-shaped relationship between sleep duration and mortality: Regularly sleeping less than five hours daily or more than nine hours raises the risk of death.1
However, analysis of electronic sleep assessment data—gathered over multiple nights using wrist bands (actigraphy)—offers a more nuanced view. Diane Lauderdale of the University of Chicago and colleagues find sleeping less than six hours per night is associated with poor or fair health among older people but sleeping longer than average is not linked to any negative health consequences.2 Their study is based on sleep data for more than 700 adults ages 62 to 90 participating in the nationally representative National Social Life, Health, and Aging Project (NSHAP). As use of “actigraphy matures, our understanding of how sleep affects health may change,” they write.
A University of California, Los Angeles team finds that one night of partial sleep deprivation activates genes related to biological aging in older adults.3 For the study, 29 older adults between ages 61 and 86 spent four nights in a sleep laboratory. Following two uninterrupted nights of sleep, participants were not allowed to sleep between 11 p.m. and 3 a.m. and later awakened at 7 a.m. Researchers monitored their sleep and drew blood daily.
After a night partially deprived of sleep, participants’ blood showed signs of deterioration in the cell’s growth and division cycle. The researchers report that these findings “causally link sleep deprivation to the molecular processes associated with biological aging,” suggesting that insufficient sleep may increase the risk of chronic disease by “activating the molecular pathways that drive biological aging.”
Michael Irwin, Richard Olmstead, and Judith Carroll of the University of California, Los Angeles, find further evidence of the effect of sleep on the aging process by analyzing results from 72 distinct studies. This body of research—involving 50,000 participants in both clinical settings and the wider population—suggests that sleep disturbances (poor sleep or insomnia complaints) and long sleep duration (sleeping more than eight hours regularly) are related to increases in blood markers of inflammation.
Specifically, disturbed sleep and too much sleep are associated with the inflammation markers C-reactive protein (CRP) and interleukin-6 (IL-6). These markers tend to be related to chronic conditions such as diabetes and cardiovascular disease. Previous research shows that treating insomnia can reduce inflammation. The researchers argue that sleep disturbance and long sleep duration should be viewed as additional risk factors for inflammation that can be modified, like high-fat diets and sedentary lifestyles. For example, several studies show that insomnia treatments can reduce inflammation markers, offering evidence that sleep problems can be a cause of inflammation.4
Poor sleep is also related to depression in old age, according to several studies.5 A University of Michigan team finds disturbed sleep is associated with depression, regardless of the number of chronic medical conditions a participant has.6> The study tracked more than 3,500 older adults participating in the nationally representative Americans’ Changing Lives Study, which surveyed participants five times over 25 years.
The researchers show that older adults diagnosed with a higher number of chronic medical conditions–such as high blood pressure, diabetes, chronic lung disease, heart attack or other heart trouble, stroke, cancer, and arthritis—have higher levels of depressive symptoms. People sleeping poorly who also have heart trouble face a particularly high risk of having depressive symptoms.
In the researchers’ view, detecting sleep problems early and intervening with medications or behavioral change is crucial, and can have long-term benefits for physical and mental health. They point out that people with depression tend to use more health care services than average, and given high medical costs, early screening and treatment of disturbed sleep may reduce costs and have “enduring public health benefits.”
Severely disturbed sleep may be an early signal of impending dementia, a team of Canadian researchers show.7 Otherwise healthy older people may experience disturbed sleep, including severe insomnia and daytime sleepiness, prior to displaying other dementia-related symptoms, such as memory loss. For the study, the researchers examined the survey responses of more than 28,000 adults ages 50 and older collected through the Survey of Health, Ageing, and Retirement (SHARE) in 12 European countries.
Using data for participants with no symptoms of Alzheimer’s disease or dementia at the beginning of the study, researchers created a sleep disturbance index (based on measures of sleep problems, fatigue, use of sleep medication, trouble sleeping, and changes in sleep patterns). Analysis shows that each separate sleep measure is independently associated with a greater risk of Alzheimer’s disease, dementia, or death within four years. After accounting for overall health, high scores on the sleep disturbance index remain associated with a greater risk of developing dementia.
Dementia is known to profoundly disrupt the sleep-wake cycle of people with the disease and leave them highly active at night, creating a burden for their family caregivers. The researchers recommend that health care providers screen for sleep problems in older people, in order to detect dementia earlier and initiate interventions to potentially prevent or delay institutionalization.
Similarly, researchers at the University of California, Berkeley show that disrupted sleep related to Alzheimer’s disease may be different from or significantly more severe than typical age-related sleep impairment.8 Evaluating older people for sleep changes linked to Alzheimer’s, such as declines in non-rapid eye movement sleep, could be a potentially non-invasive way to identify individuals at risk for Alzheimer’s disease. They suggest that sleep impairment is both “a consequence and cause of the progression of Alzheimer’s disease; one that is modifiable, offering preventative and therapeutic treatment potential.”
Dementia-related brain changes may be linked to regularly sleeping less than six hours per night and may begin in middle age, researchers based in California, Pennsylvania, Alabama, Maryland, and Illinois find.9 More than 600 black and white adults (mean age 45) in the Coronary Artery Risk Development in Young Adults (CARDIA) study reported their typical sleep duration and then had brain MRIs five years later. Compared with those who slept between six and eight hours per night, the brains of short sleepers had a greater concentration of white matter hyperintensities (a hardening of arteries in the brain), which have been linked to stroke and vascular dementia.
Subscribe to our Today’s Research on Aging newsletter by sending an email to todaysresearch@prb.org with ‘Subscribe’ in the subject line.
[1] Francesco Cappuccio et al., “Sleep Duration and All-Cause Mortality: A Systematic Review and Meta-Analysis of Prospective Studies,” SLEEP 33, no. 5 (2010): 585-92.
[2] Diane Lauderdale et al., “Sleep Duration and Health Among Older Adults: Associations Vary by How Sleep Is Measured, Journal of Epidemiology and Community Health 70, no. 4 (2016): 361-6.
[3] Judith E. Carroll et al., “Partial Sleep Deprivation Activates the DNA Damage Response (DDR) and the Senescence-Associated Secretory Phenotype (SASP) in Aged Adult Humans,” Brain, Behavior, and Immunity 51, no. 1 (2016): 223-9.
[4] Michael R. Irwin et al., “Cognitive Behavioral Therapy and Tai Chi Reverse Cellular and Genomic Markers of Inflammation in Late-Life Insomnia: A Randomized Controlled Trial,” Biological Psychiatry 78, no. 1 (2015): 721-9; and Michael R. Irwin at al., “Cognitive Behavioral Therapy vs. Tai Chi for Late-Life Insomnia and Inflammatory Risk: A Randomized Controlled Comparative Efficacy Trial,” SLEEP 37, no. 1 (2014): 1543-52.
[5] Eun Lee et al., “Persistent Sleep Disturbance: A Risk Factor for Recurrent Depression in Community-Dwelling Older Adults,” SLEEP 36, no. 11 (2013): 1685-91.
[6] Amanda Leggett et al., “The Effect of Sleep Disturbance on the Association Between Chronic Medical Conditions and Depressive Symptoms Over Time,” Longitudinal and Life Course Studies 8, no. 2 (2017): 138-51.
[7] Roxanne Sterniczuk et al., “Sleep Disturbance Is Associated With Incident Dementia and Mortality,” Current Alzheimer Research 10, no. 7 (2013): 765-75.
[8] Bryce Mander et al., “Sleep: A Novel Mechanistic Pathway, Biomarker, and Treatment Target in the Pathology of Alzheimer’s Disease?” Neuron 39, no. 8 (2016): 552-6.
[9] Kristine Yaffe et al., “Sleep Duration and White Matter Quality in Middle-Aged Adults,” SLEEP 39, no. 9 (2016): 1743-47.

By 2030, when the last of the large baby boom generation (born 1946 to 1964) has reached their mid-60s, more than 21 percent of the U.S. population is projected to be age 65 or older—up from about 15 percent in 2016.
The greying of America increases the costs of public programs for older adults and shifts the balance between working people supporting those programs and retirees receiving benefits. The old-age support ratio—the number of working-age adults ages 18 to 64 for every adult age 65 or older—is on course to shrink dramatically from 4.1 in 2016 to 2.8 by 2030. To relieve this fiscal pressure, policymakers continue to discuss new financial incentives to encourage people to postpone retirement, such as further raising the eligibility age for Social Security (currently age 67 for those born after 1960) and Medicare (now age 65).
Working longer can reduce public spending and enable some older workers to enter retirement with more financial security. Estimates based on past health trends suggest that most U.S. older adults can work an extra two years before retiring.1But a growing body of research suggests that baby boomers in their 50s and 60s are in poorer health—with more chronic disease and disability—than earlier generations at the same ages, potentially affecting their capacity to work longer.
Older adults ages 51 to 61 had a higher prevalence of six out of eight chronic conditions—including 37 percent higher diabetes prevalence—in 2004-2010 than their peers in 1992-1998, a 2016 study finds.2 Hiram Beltrán-Sánchez of the University of California-Los Angeles, Marsha Jiménez of Brown University, and S.V. Subramanian of Harvard University analyzed self-reported chronic disease in the 1990s and 2000s using data from the nationally representative U.S. Health and Retirement Study (HRS). Based on their findings, they argue that older adults nearing traditional retirement ages appear more burdened by health conditions than several decades ago.
In another recent study, a University of Southern California research team finds Americans are living longer with more disability. Eileen Crimmins, Yuan Zhang, and Yasuhiko Saito examined life expectancy trends and disability rates in the 40-year period from 1970 to 2010.3They show that the average total lifespan increased for both men and women, but so did the proportion of time spent living with a disability. For people ages 65 and older, they identify a “compression of morbidity”—that is, a reduction in the proportion of life spent with disability. However, people in their prime working years (ages 20 to 64) experienced increases in the proportion of life spent with a disability. The researchers argue that there is “little evidence” of improvements in health “that would support increasing the age at retirement.”
In addition, a 2012 study that synthesized the results of five nationally representative surveys finds increasing disability among those ages 55 to 64 between 2000 and 2008 (a group that included the oldest baby boomers).4 During the same period, disability levels continued to decline among the oldest Americans (ages 85 and older) and held steady among those ages 65 to 84.
Linda Martin of the RAND Corporation, and Robert Schoeni of the University of Michigan also document rising disability levels between 1997 and 2010 among middle-age and older Americans (ages 40 to 64).5 Their analysis, based on the nationally representative National Health Interview Survey data, identifies a link between increasing obesity and rising disability.
Martin and Schoeni take this line of research further, teaming up with HwaJung Choi of the University of Michigan for a 2016 study focusing on 55-to-69-year-olds using HRS data for 1998 to 2010.6 They find no improvement in levels of physical functioning and activity limitations during the period, and some evidence of worsening. They show that obese individuals face a greater likelihood of having physical limitations. Although baby boomers are less likely to smoke, have emphysema, or have heart attacks, they are more likely to be obese or have diabetes or high blood pressure than the previous generation at similar ages, they report.
Obesity is a risk factor for a variety of chronic conditions; it may also increase the likelihood of early retirement due to disability. Using HRS data, Francesco Renna and Nidhi Thakur of the University of Akron find that men and women under age 65 who were obese in 1992 were more likely to have a disability and retire early by 2002.7
“Obesity can largely impact labor market decisions directly through impairment of bodily functions and indirectly by being a risk factor for various diseases like hypertension, arthritis, etc.,” they write. About two in five Americans (43 percent) in their 40s and 50s were obese in 2015-2016, and thus face an increased risk of retiring early because of a disability or poor health.8
In a 2017 study, Choi and Schoeni examined trends in both physical limitations and cognitive impairment to compare the health of adults nearing retirement by generation.9 They find that adults in their late 50s today are in poorer health than their parents’ generation was at the same age, even though the younger group will have to work longer to collect full Social Security benefits.
For this study, they used HRS and National Health Interview Survey (NHIS) data and divided older Americans into five groups based on the age at which they are eligible to collect full Social Security retirement benefits: those born in 1937 or earlier (age 65); those born 1938 to 1942 (between ages 65 and 66); those born 1943 to 1954 (age 66); those born 1955 to 1959 (between ages 66 and 67), and those born in 1960 to 1962 (age 67).
They find that the younger groups had higher shares of people who had at least one limitation on their ability to perform a basic daily living task by themselves, such walking across a room, dressing, bathing, eating, and transferring into or out of bed (see figure).
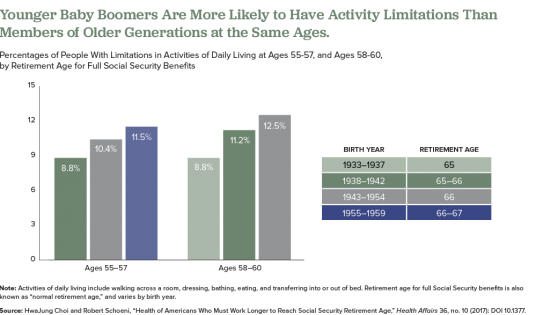
Also, they find that those born later tended to have higher rates of poor cognition, such as impaired memory and thinking ability, in their 50s compared with earlier generations at a similar age. Also, at age 50, people in the youngest group (born 1960 to 1962) were more likely to rate their own health as “fair” or “poor” than were people in the middle-three age groups when they were the same age, they report.
The researchers suggest that the increase of workers in their 50s and 60s who are in poor health will create significant challenges for them and their employers, including more people applying for Social Security disability payments. “Given the recent changes in health among the cohorts now approaching typical retirement age, further increases in the normal retirement age would place a substantial and disproportionate burden on these cohorts,” they argue.
The health of Americans in their 50s and early 60s today will shape labor force participation rates among the older population in the future. Understanding and monitoring these trends will be key as policymakers consider incentives to work longer and plan for future increases in the cost of public programs for older people.

With Americans living longer and the large baby boom generation reaching ages 65 and beyond, the sheer numbers of people with conditions of old age—including Alzheimer’s disease and other dementias—are expected to rise dramatically in coming years. But there is some potentially good news: The share of the population with dementia may have fallen over the past 25 years—likely the result of better brain health related to more schooling and aggressive treatment of high blood pressure and diabetes.
This report explores the evidence of a decline in dementia and the trends that may shape the future prevalence of this debilitating condition—focusing on recent work by researchers supported by the National Institute on Aging (NIA).
It describes what we know (and do not know) about dementia patterns, examining known risk factors and vulnerable groups. This research can guide policymakers and public health professionals as they plan for an aging population and design strategies to address health and lifestyle factors related to dementia risk.
 ">
">



 ">
">


 ">
">

 ">
">




 ">
">