Alicia VanOrman
Program Director





With the number of coronavirus infections surging, school districts across the United States are grappling with decisions about whether and how to re-open this fall. For online learning to be effective, students need access to computers and high-speed internet access, but a new analysis and interactive dashboard by PRB show sharp digital and economic divides among school-age children across states and between racial and ethnic groups.
In 2018, roughly 10% of U.S. children ages 5 to 17 did not have a computer—desktop, laptop, or tablet—at home, and 23% did not have home access to paid high-speed internet.1 Fully one-fourth of all school-age children were lacking either a computer or high-speed internet. Children without computers or high-speed internet at home were already at an educational disadvantage before the COVID-19 pandemic due to the growing need for students to access resources and submit assignments online. Many relied on computers and internet access at school or a local library to complete their work. As the pandemic prompted libraries to close and schools across the country shut down and moved to online instruction, this digital divide has become even more critical.
A racial and ethnic digital divide also persists. Half of all American Indian/Alaska Native children lack either computers or paid high-speed internet access (or both) at home (see Table 1). More than one-third of Black and Latinx children lack computers or high-speed internet at home, compared with only one-fifth of non-Hispanic white children and one in seven Asian/Native Hawaiian and Other Pacific Islander (NHOPI) children.
Economic barriers contribute to the digital divide between racial and ethnic groups. Poverty rates range from 10% among non-Hispanic white children ages 5 to 17 to 31% among Black children. American Indian/Alaska Native and Latinx children also have poverty rates far above the national average of 17%.
Black, American Indian/Alaska Native, and Latinx school-age children are two to three times more likely to live in households receiving Supplemental Nutrition Assistance Program (SNAP) benefits than white or Asian/Native Hawaiian and Other Pacific Islander children. Nearly 40% of Black and 35% of American Indian/Alaska Native school-age children live in households receiving SNAP benefits. Children whose households receive SNAP benefits are automatically eligible to receive free meals at school—which provide an essential source of daily nutrition for many of these children. With schools shut down, children of color whose families live in poverty and receive SNAP benefits are at much greater risk of going hungry and not receiving the nutrition they need during the pandemic.
Digital and Economic Divides of Children Ages 5 to 17 by Race and Ethnicity, 2018
| wdt_ID | Racial or Ethnic Group | Lacks Computer, High-Speed Internet Access, or Both | Family Income Below 100% of Poverty | Household Receives SNAP Benefits |
|---|---|---|---|---|
| 1 | American Indian/Alaska Native | 50 | 30 | 35 |
| 2 | Black | 36 | 31 | 39 |
| 3 | Hispanic or Latino | 34 | 25 | 28 |
| 4 | White | 20 | 10 | 12 |
| 5 | Asian/NHOPI | 14 | 11 | 11 |
| 6 | Two+ Races | 19 | 16 | 23 |
| 7 | All Children | 25 | 17 | 21 |
Nearly half (47%) of school-age children who live in poverty and 43% of those who receive SNAP benefits lack access to either computers or high-speed internet, compared with only 21% of children who do not receive SNAP benefits and whose family incomes are above the poverty line.
Within every racial and ethnic group, the share of school-age children without access to computers or high-speed internet is much higher for those who receive SNAP benefits and those who live in poverty (see Figure 1). While half of all American Indian/Alaska Native children lack access to computers and high-speed internet, this share jumps to 61% for those receiving SNAP benefits and nearly 70% among those living in poverty. Among non-Hispanic white children, the share without access to computers and high-speed internet nearly doubles from 20% to 39% for those receiving SNAP benefits and from 20% to 41% for those in poverty. Lower levels of economic well-being are widening racial and ethnic gaps in access to computers and high-speed internet.
Percent of Children Ages 5 to 17 in Different Racial/Ethnic Groups Lacking Access to Computers or High-Speed Internet by Poverty Status and Receipt of SNAP Benefits, 2018
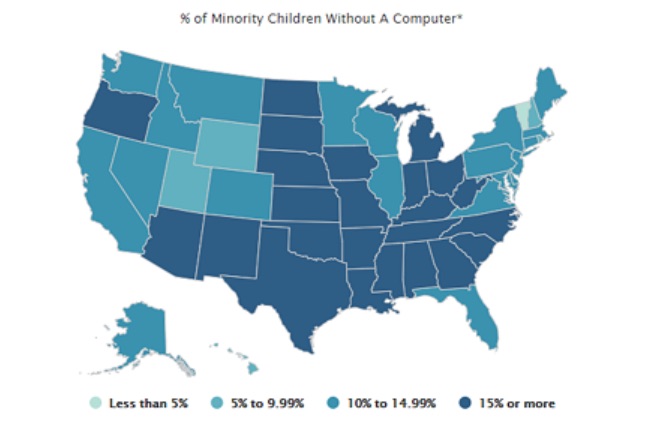
States vary widely in their shares of school-age children without access to computers and high-speed internet, from a low of 13% in New Hampshire to a high of 46% in Mississippi. In eight states—Alabama, Arkansas, Louisiana, Mississippi, New Mexico, Oklahoma, Tennessee, and Texas—more than 30% of children lack either or both computers and internet access, but this count rises to 31 states (including the District of Columbia) for minority children. More than half of school-age minority children in Mississippi, Arkansas, and South Dakota lack access to computers and high-speed internet at home.2
The economic divide is also present in every state. Twelve states (including the District of Columbia) have more than 20% of children ages 5 to 17 living in poverty, and 24 states (including the District of Columbia) have more than 20% of school-age children living in households receiving SNAP benefits. Concentration of poverty and SNAP receipt among school-age minority children is much higher than among non-minority children and is widespread across states. There are only 10 states where the share of minority children living in poverty drops below 20% and only three states (Utah, Vermont, and Wyoming) where the share in households receiving SNAP benefits falls below 20%. Conversely, nine states (Alabama, Arkansas, Louisiana, Mississippi, Ohio, South Carolina, South Dakota, Tennessee, and West Virginia) have one-third or more of minority school-age children living in poverty, and 22 states have more than one-third living in households receiving SNAP benefits.
Digital and economic divides among school-age children are linked to differences in reading and mathematics proficiency levels across states and between racial and ethnic groups. Proficiency in reading by the end of third grade is an important marker of overall educational development but, beginning in fourth grade, it is also essential for learning other subjects and keeping up academically.3 Children who reach fourth grade without being able to read proficiently are more likely to drop out of high school—reducing their earnings potential and chances for success.4 Similarly, proficiency in mathematics fundamentals makes college attendance and completion more likely, which increases earnings potential.5
In 2019, a shocking two-thirds of all fourth graders in the United States scored below the proficient level in reading, as did two-thirds of eighth graders in math. However, these shares are much higher among children in the racial and ethnic groups with the highest levels of poverty and receipt of SNAP benefits, and the least access to computers and high-speed internet (see Figure 2).
Reading and Math Proficiency of Children by Race and Ethnicity, 2019
Among Black and American Indian/Alaska Native students, at least 80% of fourth graders scored below the proficient level in reading, and 85% or more of eighth graders scored below the proficient level in math. More than three-quarters of Latinx fourth graders scored below the proficient level in reading and math in 2019. With higher levels of economic well-being and access to computers and high-speed internet, the shares of non-Hispanic white and Asian/Native Hawaiian and Other Pacific Islander children scoring below the proficient level in reading and math are much lower. These gaps in basic reading and math skills make it hard to envision how today’s children can become tomorrow’s productive workers in a globally competitive economy. In outlining his education policy in 2009, President Barack Obama argued that “The relative decline of American education is untenable for our economy, it’s unsustainable for our democracy, and it’s unacceptable for our children—and we cannot afford to let it continue.”6
States also vary widely in reading and math proficiency levels. For example, the share of fourth graders who scored below the proficient level in reading ranged from a low of 55% in Massachusetts to a high of 76% in New Mexico, while at least seven out of 10 children scored below proficient in reading in eight states. The share of eighth graders who scored below proficient in math ranged from a low of 53% in Massachusetts to a high of 79% in New Mexico, while at least seven out of 10 eighth graders scored below the proficient level in math in 17 states in 2019.
The low levels of proficiency in reading and math among children of color are even more concerning given the fact that minorities make up a growing share of the school-age population. The share of school-age children who are members of a racial or ethnic minority ranges from a low of 7% in Vermont to a high of 80% in the District of Columbia. Among minority students, only two states—Hawaii and Vermont—had fewer than seven out of 10 fourth graders who scored below the proficient level in reading. However, no states had fewer than seven out of 10 minority eighth graders who scored below proficient in math. For example, nearly half (48%) of school-age children in Louisiana belong to a racial or ethnic minority group, and 84% of minority fourth graders scored below proficient in reading while 88% of minority eighth graders scored below proficient in math. Taken together, roughly 40% of all fourth and eighth graders in Louisiana had already fallen behind academically even before the COVID-19 pandemic hit and schools closed.
As schools shut down in spring 2020, some districts like Los Angeles Unified tried to address the digital divide by distributing laptops to all students who needed them. In addition, some districts provided internet access to students without it by distributing hot spots or data plans. However, these solutions were not economically feasible in many districts serving low-income communities of color such as Prince George’s County Public Schools in Maryland. With 10 of the 15 largest school districts already deciding to begin the new school year online as of early August, reducing the digital divide and providing free and reduced-price meals for children who need them has become a daunting challenge across the country.
Unemployment rates remain at record highs, and with the supplemental $600 unemployment payments ending and Congress unable to agree on a new stimulus package, poverty levels and demand for SNAP benefits are both likely to rise this fall. A growing economic divide may further exacerbate the digital divide among school-age children, putting even more students at risk of falling further behind.

The past two decades have been tumultuous for the United States. During the first 20 years of the 21st century, the nation experienced a major terrorist attack, a housing market meltdown, a severe economic recession, a significant downturn in the stock market, and a pandemic that led to the highest unemployment rate since the Great Depression.
The coronavirus and the disease it causes, COVID-19, are affecting all Americans. Older people are most at risk of severe health issues related to the virus, but young adults—ages 25 to 34—may be most vulnerable to its long-term social and economic impacts. Those in their early 30s reached young adulthood during the Great Recession of 2007 to 2009 and experienced one of the most challenging job markets in U.S. history. Now those in their mid-20s are entering prime marriage and family formation years just as the coronavirus pandemic is causing extensive economic and social disruptions.
Even before the crisis hit, more young Americans had been postponing key life events that often mark the transition to adulthood. Fewer young adults in their 20s and 30s are getting married, having children, living independently from their parents, buying homes, and achieving financial independence. Nearly one in five young adults ages 25 to 29 are disconnected from work and school. A growing share of young adults carry high levels of student loan and credit card debt that may cause them to postpone marriage and family formation.1 The pandemic will likely amplify these trends.
The statistics are grim. More than 40 million workers filed for unemployment benefits in the spring of 2020. Millions of young adults work in restaurants and other service-sector jobs that have been heavily affected by stay-at-home orders and social distancing measures. The pandemic is also exacerbating the wide economic disparities between whites and other groups—especially Blacks and Latinos—who are more likely to be working in low-wage jobs with few benefits.
The current health and economic crisis is unprecedented, making it difficult to predict the impact on patterns of marriage, childbearing, homeownership, and living arrangements of young adults in the coming months and years. But we can look back at recent trends for clues.
While the Great Recession may have forced some young adults to postpone key life transitions—such as finding a full-time job or buying a home—the decline in the proportion who are married is a longer-term trend that predates the economic downturn. It’s hard to gauge whether the decline in marriage during the recession was due to economic factors or just a continuation of previous trends.
The coronavirus may be different. In the short term, it will force millions of young adults to consider postponing marriage until social distancing restrictions are lifted. Longer-term effects on marriage are more difficult to predict.
On the one hand, some young adults—particularly those with less education and lower incomes—may decide to postpone marriage until the economy recovers, which could take years. The “economic prerequisites for entering marriage are higher today than they were for previous generations.”2 Meeting those requirements—finding a job, achieving some financial independence, accumulating some savings, and perhaps buying a home—may be harder than ever in the current environment, especially for lower-income workers without college degrees.3
The decline in the proportion married among young adults with lower levels of education accelerated during the Great Recession and has continued over the past decade (see Figure 1). The proportion of college graduates who are married has also declined but at a slower pace, which has led to a growing marriage gap between those at different education levels.4
FIGURE 1. Share of Young Americans Ages 25 to 34 Who Are Married (Spouse Present), by Educational Attainment, 2000-2025
Note: Projections are calculated by applying the average rate of change during the Great Recession and its aftermath to future years.
Source: IPUMS-Current Population Survey, University of Minnesota, www.ipums.org.
Between 2000 and 2019, the proportion of young adults without bachelor’s degrees who were married dropped 16 percentage points to 37%. But for college graduates, the proportion dropped just 10 percentage points to 46%. The fallout from the coronavirus could exacerbate the marriage gap for people at opposite ends of the education ladder.
If patterns since the Great Recession continue, about one-third (32%) of young adults without bachelor’s degrees may be married by 2025, compared with 42% of young adult college graduates.
On the other hand, marriage provides an opportunity to pool resources and offers tax and health coverage benefits that may be attractive to some young adults who were on the fence about tying the knot.5 A key factor contributing to the recent decline in marriage rates, especially for less-educated groups, has been the rise in women’s earnings relative to men.6 As women’s wages have increased, fewer women have relied on a spouse or partner to provide a paycheck. However, the current economic crisis may disproportionately affect women, who are more likely to be employed in service-sector jobs. A rise in “marriageable men” relative to women could potentially lead to an increase in the proportion of young adults who marry in the coming years.7
As marriage rates among young adults have declined in recent years, cohabitation rates have increased, either as a precursor to or substitute for marriage.
The share of young women ages 25 to 34 living with a partner more than doubled between 2000 and 2019, from 7% to 22% (see Figure 2). For men, cohabiting increased from 8% to 19% during the same period. The share of young adults who have ever cohabited is much higher and increasing. In 1995, nearly half (49%) of women ages 25 to 29 had ever cohabited, but that share rose to 73% in 2011 to 2013.8
FIGURE 2. Share of Young American Men and Women Ages 25 to 34 Living With a Cohabiting Partner, 2000-2025
Notes: A change in methods used to identify cohabiting couples accounts for part of the increase in cohabitation in 2007. Projections are calculated by applying the average rate of change during the Great Recession and its aftermath to future years.
Source: U.S. Census Bureau, Current Population Survey.
Cohabiting relationships in the United States tend to be short, with most couples breaking up or getting married within a few years. Serial cohabitation—a pattern of multiple, nonmarital cohabiting relationships—is also increasingly common, especially among couples with lower levels of education.9
Will more young adults choose to live together because of the coronavirus pandemic’s impact on the economy? In the short term, anecdotal evidence suggests that social distancing measures have “fast-tracked many relationships” among couples forced to choose between living separately indefinitely and moving in together.
Other couples may decide to postpone cohabiting until economic prospects improve. Population Reference Bureau projections indicate that the share of young adult women and men who are cohabiting could rise to 22% and 19%, respectively, by 2025.
Some have speculated that the coronavirus pandemic will lead to a baby boom, with so many couples stuck at home due to social distancing requirements. But the research suggests otherwise.
The U.S. total fertility rate (TFR) has declined during previous economic downturns, and the current economic crisis will likely have a similar impact on births. The TFR fell to low levels during the Great Depression in the 1930s, amid the 1970s oil shock, and with the Great Recession in 2007. Fertility in the United States recently dropped to the lowest level in recorded history, with women having an average of 1.7 births in their lifetime.
The timing of childbearing has also changed. Delays in marriage have in turn resulted in delays in first births. In 2018, the average age of first-time mothers was 27, up from 25 in 2000. By 2016—for the first time in U.S. history—the birth rate among women ages 30 to 34 (103 births per 1,000 women) exceeded that of women ages 25 to 29 (102 births per 1,000 women) (see Figure 3).
FIGURE 3. U.S. Births per 1,000 Women, by Age Group, 2000-2025
Note: Projections are calculated by applying the average rate of change during the Great Recession and its aftermath to future years.
Source: U.S. Centers for Disease Control and Prevention, National Center for Health Statistics.
The economic impact of the coronavirus may cause more young adults to postpone births, leading to further declines in birth rates, especially among women under age 30.
States like Nevada, which relies heavily on tourism, may see bigger declines in fertility than states with more diversified economies. Fertility declines during the Great Recession were greatest in states most impacted by the economic downturn.10
Searching for a home right now is challenging because of social distancing guidelines, but the longer-term effects of the coronavirus on the housing market could linger for years. Millions of Americans who have been temporarily or permanently laid off may lose income and have to dip into their savings, decreasing their ability to secure a loan or make a down payment on a house. Many existing homeowners may need to sell their homes to help pay the bills.
The homeownership rate among young adults declined with the onset of the subprime mortgage crisis in 2007 and has continued to drop (see Figure 4). Between 2007 and 2019, householders ages 65 and older experienced a modest decline in homeownership (1 percentage point), whereas rates dropped sharply for householders ages 25 to 34 (8 percentage points) and 35 to 64 (9 percentage points).
FIGURE 4. U.S. Homeownership Rates by Age of Householder, 2000-2025
Note: Projections are calculated by applying the average rate of change during the Great Recession and its aftermath to future years.
Source: IPUMS-Current Population Survey, University of Minnesota, www.ipums.org.
Historically, young adults (ages 25 to 34) have had lower homeownership rates than adults ages 65 and older, and the gap between these two groups has increased 4 percentage points from 2000 to 2019. By 2025, this gap could grow even wider, according to PRB’s projections. By 2025, just 34% of householders ages 25 to 34 may be homeowners, compared with 80% of householders ages 65 and older.
Although this trend may suggest a change in housing preferences, more than two-thirds of renters report that they would buy a home if they had the financial resources to do so.11 The decline in homeownership has also been linked to lower rates of marriage and family formation among young adults.12 The share of young men and women ages 25 to 34 living with a spouse dropped from 50% and 57%, respectively, in 2000 to 36% and 45%, respectively, in 2019.13
Wide gaps in homeownership rates also persist across different racial and ethnic groups. During the housing market crisis, owning a home became a liability for many Americans but especially for African Americans and Latinos, who were more likely to have high-cost or subprime mortgages. Black and Latino workers were disproportionately low income prior to the coronavirus pandemic, and the current economic crisis could further impact the ability of Black and Latino young adults to qualify for loans or make their mortgage payments in the coming months.
Declines in marriage have been accompanied by an increase in young adults—especially men—returning to or remaining in their parents’ homes, and the coronavirus pandemic will likely intensify this trend.
Between 2000 and 2019, the share of young men ages 25 to 34 living with their parents rose from 12% to 22% (see Figure 5). The share of young women living with their parents increased from 8% to 15% during the same period. For both men and women, the proportion who were doubling up with their parents in 2019 was at or near the highest levels since the U.S. Census Bureau first started tracking the measure in 1960.
FIGURE 5. Share of Young American Men and Women Ages 25 to 34 Living With Their Parents, 2000-2025
Note: Projections are calculated by applying the average rate of change during the Great Recession and its aftermath to future years.
Source: U.S. Census Bureau, Current Population Survey.
The rising number of young adults living with their parents, often disconnected from work and school, may lead to further declines in marriage, family formation, and childbearing. About 22% of young men and 15% of young women are projected to be living in their parents’ homes by 2025.
The coronavirus pandemic could be the most significant event that will occur in our lifetime and will likely have long-lasting effects on marriage, family formation, poverty, and health in the United States. Some have pointed to the positive effect of the pandemic on bringing families together, but researchers have also shown that entering the job market during a period of economic turmoil can have long-term, negative consequences for young adults. In midlife, they earn less (while working more), are less likely to be married, are more likely to be childless, and are more likely to die prematurely compared with young adults who enter the workforce during a healthier economy.14 Young adults who entered the job market during the Great Recession are still feeling the impact.
Blacks and Latinos have been disproportionately affected by layoffs due to the pandemic, and the negative effects on Black and Latino young adults will likely linger for years—exacerbating long-standing social, economic, and health inequalities between whites and other racial/ethnic groups.
Right now, life is on hold for millions of Americans. We cannot predict the long-term effects of this crisis, but it’s likely that young adults will be severely impacted by the economic fallout. Making sure these young adults have the resources they need to cover their basic needs and access educational, employment, and training opportunities—both during and after the pandemic—will be an ongoing challenge for federal, state, and local policymakers for many years.

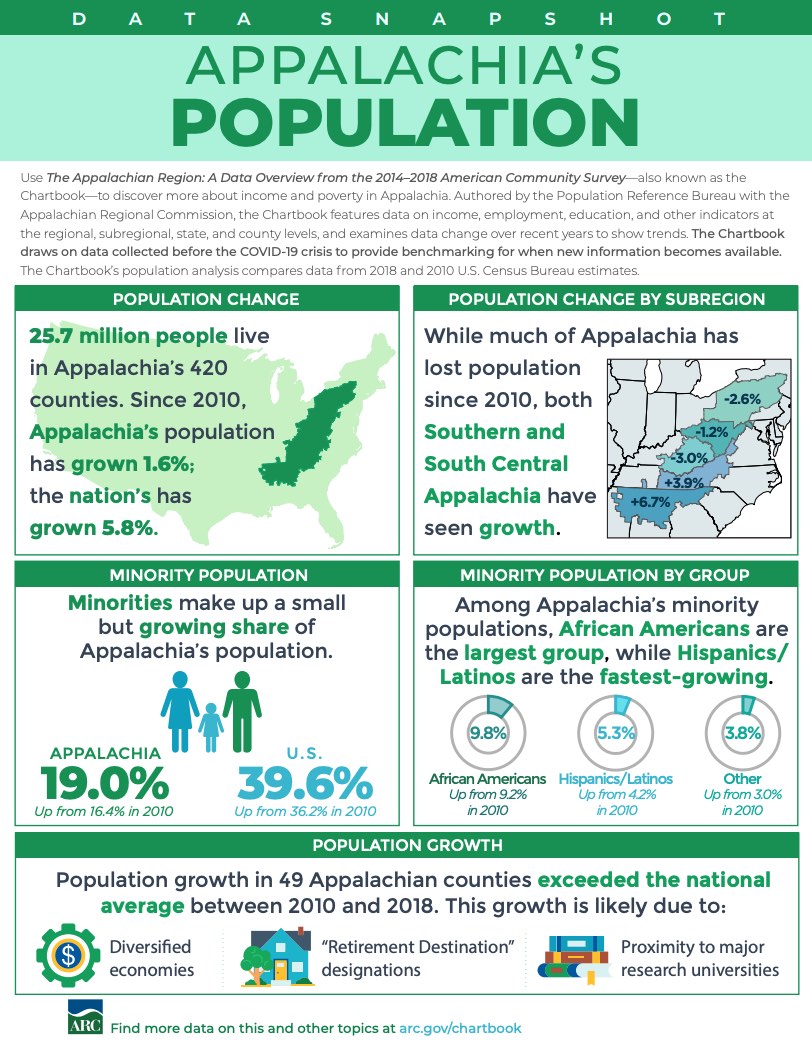
Although Appalachia’s residents of nearly all ages have been more likely to have health insurance than other Americans in recent years, the Region may be more vulnerable to the health and schooling impacts of the coronavirus pandemic due to larger shares of elderly and disabled residents and lower levels of computer and broadband access.
The Appalachian Region: A Data Overview From the 2014-2018 American Community Survey (51 MB), a Population Reference Bureau (PRB) report for the Appalachian Regional Commission, provides a comprehensive picture of social and economic conditions in Appalachia prior to the coronavirus pandemic. These data can help researchers and policymakers assess the pandemic’s potential implications for the Region.
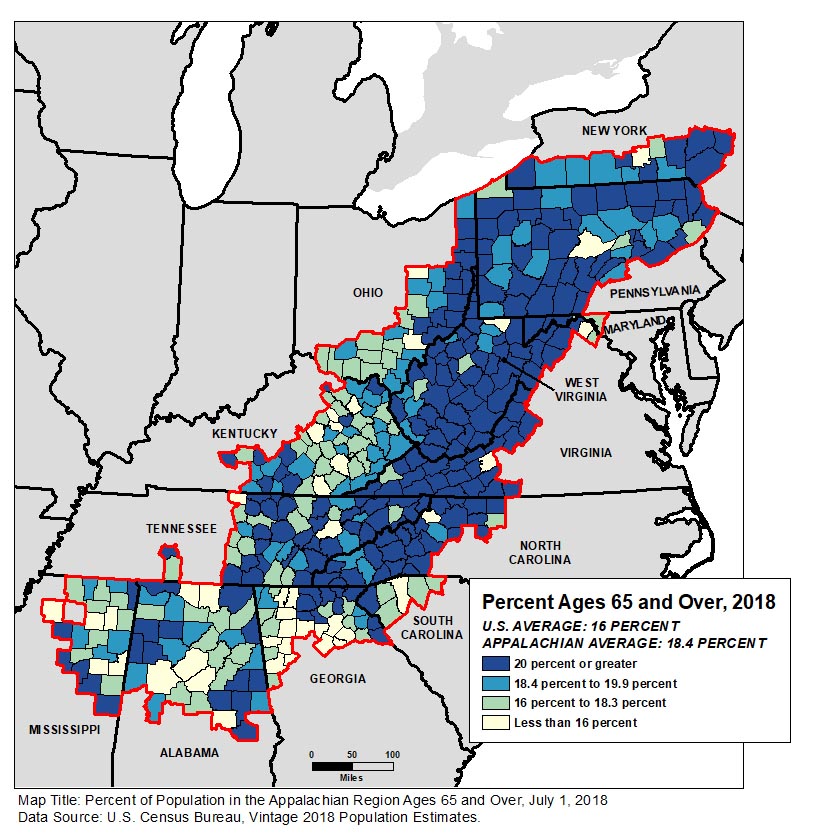
People ages 65 and older made up 18.4% of Appalachia’s population—more than two percentage points above the national average. The share exceeded 20% in more than half of the Region’s counties (see Figure 1).
Among all age groups, the share of Appalachian residents who reported a disability (difficulty with hearing, vision, cognition, walking or climbing, self-care, or independent living) in 2014-2018 was above the national average—with the widest gap among 35- to 64-year-olds (more than four percentage points: 17.1% in Appalachia versus 12.8% nationwide).
“People ages 65 and over and those with underlying health conditions are considered among the groups most vulnerable to serious complications related to the coronavirus; if the virus becomes widespread in Appalachian communities with the largest share of older adults, they may risk high illness and death rates,” says Kelvin Pollard, PRB senior demographer and report co-author.
Just over 84% of Appalachian households had access to a computer device, nearly five percentage points below the national average. The share of households with broadband access, at 75%, was likewise five points below the national average. The report found that the digital divide was particularly acute in Appalachia’s most rural communities: three in 10 rural Appalachian households lacked internet access.
“With most schools closed due to the coronavirus pandemic, this rural digital divide has made online education and maintaining learning extremely challenging,” according to report co-author Linda A. Jacobsen, PRB’s vice president for U.S. Programs.
The report also compares Appalachia’s 107 rural counties (that is, counties that are neither part of nor adjacent to a metropolitan area) to the 840 rural counties outside the Region. It shows that rural Appalachia lagged behind the rest of rural America on a variety of measures such as educational attainment, household income, population growth, and labor force participation.
However, residents of rural counties in Appalachia were more likely than residents of rural counties outside the Region to have health insurance coverage in the 2014-2018 period—both among all residents and among young adults ages 26 to 34 where noncoverage rates were highest.
But disability rates and poverty rates were also significantly higher in rural Appalachia than in other parts of rural America (see Figure 2). Disability rates in Appalachia were higher in every age group, with a six-percentage point gap among those ages 35 to 64 and ages 65 and older.
| wdt_ID | Population | Appalachian Rural | Non-Appalachian Rural |
|---|---|---|---|
| 1 | With a Disability | 20 | 16 |
| 2 | Adults 18-64 With a Disability | 18 | 14 |
| 3 | Adults 35-64 With a Disability | 23 | 17 |
| 4 | Adults 65+ With a Disability | 44 | 38 |
| 5 | In Poverty | 22 | 16 |
| 6 | Children in Poverty | 30 | 23 |
| 7 | Adults 18-24 in Poverty | 32 | 26 |
| 8 | Adults 25-64 in Poverty | 20 | 14 |
| wdt_ID | Population | Appalachian Rural | Non-Appalachian Rural |
|---|---|---|---|
| 1 | In Poverty | 22 | 16 |
| 2 | Children in Poverty | 30 | 23 |
| 3 | Adults 18-24 in Poverty | 32 | 26 |
| 4 | Adults 25-64 in Poverty | 20 | 14 |
Poverty rates in rural Appalachia were also higher, with at least a six-percentage point gap in every age group. Nearly one-third of young adults ages 18 to 24 were in poverty in rural Appalachia in 2014-2018—a rate even higher than that among children.
“Across the country, lower-income households and young adults have been hard hit by the current pandemic in terms of job and income loss; our findings indicate that conditions were already more challenging in rural counties within Appalachia than in those outside the Region, even before the pandemic,” said Jacobsen.
The Appalachian Region encompasses 205,000 square miles along the Appalachian Mountains from southern New York to northern Mississippi, including portions of 12 states and all of West Virginia. The Appalachian Regional Commission report uses data from the 2014-2018 American Community Survey and the Census Bureau’s vintage 2018 population estimates—the most recent data available for the characteristics studied. It includes detailed tables and county-level maps covering state- and county-level data on population, age, race and ethnicity, housing occupancy and tenure, housing type, education, computer ownership and internet access, labor force participation, employment and unemployment, transportation and commuting, income and poverty, health insurance coverage, disability status, migration patterns, and veteran status. It also includes a detailed comparison of characteristics in rural Appalachian counties with those outside the Region.
The Appalachian Regional Commission is an economic development agency of the federal government and 13 state governments focusing on 420 counties across the Appalachian Region. ARC’s mission is to innovate, partner, and invest to build community capacity and strengthen economic growth in Appalachia to help the Region achieve socioeconomic parity with the nation.

Since then, it has spread at an alarming rate, with more than half of countries in the region now experiencing community transmission—when new cases occur without any known contact with someone from an infected area.1 South Africa leads the region with nearly 40,800 confirmed cases as of this writing, followed by Nigeria (11,500), Ghana (8,900), and Cameroon (7,400).2
Although the region is still reporting fewer cases of COVID-19 than the rest of the world, the wide geographic spread of infection suggests a large number of unreported cases and deaths. In addition to governance and health system structures, other regions’ experiences offer general models for how the pandemic may play out, but sub-Saharan Africa’s specific characteristics related to age, health, and lifestyle will affect its trajectory in both positive and negative ways. Here’s what we’re keeping an eye on as we monitor the pandemic in collaboration with our partners in the region.
Evidence shows that older populations are hardest hit by the coronavirus. Sub-Saharan Africa has a much younger population than China, the United States, the European Union, and other areas already experiencing widespread infection. The median age is 38 in China and the United States, and 43 in the European Union, but it is just under 20 in sub-Saharan Africa.3
Only 3% of the region’s population is over age 65, the threshold for significantly higher risk of COVID-19-related complications and death.4 In Italy, which has had one of the highest COVID-19 mortality rates in the world, 23% of the population is over age 65. In contrast, in Nigeria, Africa’s most populous country, 44% of the population is under age 15—a group that has thus far been spared the worst of the pandemic (see figure).
According to modeling by the Center for Global Development, assuming a worst-case infection scenario without government intervention, 1.3% of Spain’s population would be killed by the epidemic compared to 0.15% of Uganda’s based on differences in the country’s age distribution alone (assuming the relationship between age and mortality and all other factors are the same).5 While we know that health and other factors come into play, sub-Saharan Africa’s youthful age structure could contribute to a lower regional mortality rate.
FIGURE. Sub-Saharan African Countries Have a Much Younger Age Profile Than European Countries
Sources: PRB analysis of data by the United Nations, World Population Prospects: 2019 Revision.
Other demographic features in sub-Saharan Africa, however, could complicate prevention and mitigation efforts related to COVID-19.
Migration. When people travel the continent by land and air, they pose a significant risk of carrying the coronavirus with them, undetected, into neighboring countries. South Africa, Kenya, and Ethiopia are travel hubs for the rest of the continent, creating a situation where people may move from higher prevalence areas to lower prevalence areas, driving the spread of infection. When South Africa declared its lockdown in late March, for example, it sent 14,000 Mozambican workers back across the border.6 West Africa is particularly vulnerable, having both the most migrants and the most reported cases of COVID-19 as of this writing.7
Displaced persons. The United Nations Refugee Agency reported in 2019 that sub-Saharan Africa hosts more than 17 million internationally displaced persons and six million refugees—more than a quarter of the world’s refugee population.8 Such a high number of displaced persons, who are more likely to live in close quarters with others and often in conditions with poor sanitation and hygiene, limits countries’ abilities to monitor infection rates and enforce preventative measures such as physical distancing.
Rapid urbanization. Physical distancing is challenging in urban areas with high population density. These difficulties are especially acute in sub-Saharan Africa, which is experiencing the fastest rate of urbanization in the world and anticipating 65 million additional urban residents each year.9 More than half the region’s city dwellers live in slums or informal housing known for unhygienic and crowded conditions, and 63% of city residents lack access to clean water and soap for frequent handwashing.10 As a result, basic precautions against COVID-19 recommended by the World Health Organization may not be feasible for a large portion of the population.11
Large households. With an average household size of 6.9 people, multigenerational households are more common in this region than in any other.12 Such housing arrangements—in close quarters with children and working adults—could put older individuals at heightened risk of infection and death from COVID-19. In West African countries such as the Gambia and Senegal, for example, households with at least one older family member had an average of 12 residents.13 Even when at-risk individuals can avoid nonessential interactions outside the home, their family members pose an infection risk in shared spaces.14
Experience with other infectious disease outbreaks has given some countries in sub-Saharan Africa a head start in terms of preparedness and health infrastructure to slow the spread of the coronavirus. In late February 2020—nearly a month before countries in the region implemented widescale social distancing measures—the new Africa Centres for Disease Control created a continental plan to train health care workers in 48 countries to process coronavirus tests.15
At country levels, recently established and strengthened public health organizations such as the Nigeria Centers for Disease Control have redirected existing disease task forces and resources to the coronavirus containment effort.16 Resuming procedures established for the 2014 Ebola crisis, for example, the Democratic Republic of the Congo (DRC) swiftly implemented screening, testing, and contact-tracing procedures and readied its bio-secure emergency care units.17 Uganda, which has operated in a state of health care emergency since 2018, mobilized border surveillance teams and screened travelers at its principal international airport using surveillance staff and thermometers on hand from combatting past diseases such as yellow fever, measles, and the Crimean-Congo hemorrhagic fever.18
These early preparedness measures may help countries in the region slow and contain the spread of the coronavirus.
Existing health conditions. Aside from age, a person’s overall health plays a major role in determining how COVID-19 symptoms manifest. In sub-Saharan Africa, a wide range of diseases have wreaked havoc on individuals’ immune systems. Specifically, infectious diseases such as HIV/AIDS and tuberculosis disproportionately affect people in the region and may potentially put the population at higher risk of suffering severe complications from COVID-19, especially if treatments for these diseases are interrupted. In 2018, the region claimed 24% of the 10 million cases of tuberculosis, including 72% of co-infection cases in vulnerable HIV-positive individuals.19 Sub-Saharan Africa is home to two-thirds of people living with HIV worldwide.20 Notably, 89%, or 1.5 million of the 1.6 million adolescents living with HIV worldwide, are in sub-Saharan Africa—a vulnerability that could potentially erode Africa’s otherwise youthful advantage against the coronavirus.21 Research has shown that adolescents have particular difficulty adhering to the treatment regimens that suppress HIV, making them more vulnerable to other infections.22
The region also has high rates of noncommunicable diseases (NCDs), which have grown substantially in recent decades as a proportion of the total disease burden. The single largest category of NCDs are cardiovascular diseases such as ischemic heart disease, hypertension, and high blood pressure, all of which increase the risk of becoming severely ill from COVID-19.23 High rates of smoking and unhealthy diets, common in African countries with relatively higher rates of urbanization, also contribute to this health burden. Recent studies estimate that 5% of sub-Saharan Africans have diabetes and 20% are obese.24 In addition, individuals develop NCDs at much younger ages in sub-Saharan Africa than in high-income countries, PRB reports, possibly exacerbating the pandemic’s impact on the region.
“Critical immunization programs and malaria prevention activities have been sidelined as health care workers and resources are diverted to combat the COVID-19 pandemic.”
Health systems capacity. Despite its past experiences with disease outbreaks, the region’s limited health care infrastructure, including weak supply chains, shortages of health personnel, and low testing and laboratory capacity, will make it difficult to respond to the coronavirus pandemic. Public health care spending in Africa is among the lowest in the world, with an estimated $66 billion in unmet needs, according to one study.25 Although health care capacity varies widely among sub-Saharan African countries, on average, the region has only 0.2 doctors for every 1,000 people compared with 1.8 in China and 3.7 in the European Union.26
Many health care facilities in the region lack electricity and essential medicines, and few countries have sufficient intensive care units (ICUs) to treat the critically ill.27 Uganda has just 0.1 ICU beds for every 100,0000 people.28 The United States, where many hospitals are at risk of reaching capacity with COVID-19 patients, has 35 ICU beds. The supply of ventilators is further restricted. Even fewer countries in sub-Saharan Africa have enough ventilators, the life-saving equipment required to treat the most severe cases of COVID-19. As of March 2020, for example, Liberia did not have a single ICU equipped with ventilators. An International Rescue Report in April 2020 found that South Sudan had four ventilators for its population of 11 million and Burkina Faso had 11 ventilators for its 20.9 million people.29
Although international aid is helping close these gaps, all external sources of funding and resources will be constrained as the coronavirus spreads around the world. And as health facilities ration supplies of personal protective equipment for COVID-19 cases, their capacity to care for patients with tuberculosis and other infectious diseases will decline.30 Critical immunization programs and malaria prevention activities have been sidelined as health care workers and resources are diverted to combat the pandemic.31
Most sub-Saharan Africans cannot work from home or practice physical distancing in their jobs because of the kinds of work they do. Seventy-seven percent of non-farm employment in the region is informal, the highest percentage in the world.32 Small business owners, merchants, and vendors who rely on income from each day’s work to meet basic needs for themselves and their families—without employment benefits or social protection—cannot easily abide by government directives like shelter-in-place orders.
Some countries have introduced measures to lessen the economic impact of the coronavirus restrictions and incentivize distancing, including emergency cash payments to the recently unemployed in Namibia and Cabo Verde and widespread tax relief in Kenya.33 These efforts are relatively minor, however, and will be difficult to sustain in the wake of future pandemic-related economic shocks and market interruptions. The potential for public income support that can encourage people to stay at home is extremely limited for most countries because of underfunding of social programs and high levels of public debt.
In light of these conditions, COVID-19 mitigation strategies are being adapted for the sub-Saharan African context. Many African countries have already implemented physical distancing measures such as curfews, city lockdowns, and travel restrictions. Nigeria, Zimbabwe, and South Africa were some of the earliest countries to initiate lockdowns that limited travel and closed nonessential businesses.34 Across the continent, many places of worship have closed their doors or implemented outdoor services that comply with physical distancing requirements.
In some places, however, social resistance to preventative measures threaten the success of curfews and lockdown measures.35 Protestors have had violent clashes with police in Kenya and South Africa over restrictions.36 In Malawi, personal rights concerns have led high courts to block lockdown measures from being enacted until a social safety net is in place.37 Ghana, the DRC, and other countries began easing restrictions early on in response to economic hardships and what they perceived as slow rates of infection, followed by South Africa beginning in early June.
Balancing health and economic considerations is an enormous challenge for every country battling this pandemic, but sub-Saharan Africa’s unique characteristics mean that countries might pursue different strategies than those adopted in other regions. Monitoring how the region’s demography and health characteristics shape the course of the pandemic, and exchanging lessons learned across countries with similar profiles, is critical for policy and program responses to integrate the latest evidence.
The authors would like to thank Kaitlyn Patierno, Barbara Seligman, Lara Vaz, and Laura Wedeen for their helpful comments and suggestions. We also appreciate the research support provided for this article by Omaris Caceres, Elaine Les, and Kate Rogers from Georgetown University.

Loneliness makes us focus on ourselves but redirecting that focus outward… can change our outlook, our brains, and our body chemistry.
Steve Cole, Professor of medicine and biobehavioral sciences at the University of California, Los Angeles








 ">
">










 ">
">